
ADVERTISEMENT
You do not have any notes added to this page yet
Liver cirrhosis
Nutritional and metabolic disorders
Inflammatory bowel disease
Vascular disorders
Bowel-associated dermatosis-arthritis syndrome
Hereditary gastrointestinal tumours
Paraneoplastic syndromes associated with gastrointestinal malignancies
Dermatological symptoms and signs sometimes precede or accompany a gastrointestinal disease. It should be noted that the embryonic origin of the gastrointestinal tract and the skin are closely aligned.
Common cutaneous manifestations of liver cirrhosis include:



Malnutrition associated with deficiencies of fat-soluble and water-soluble vitamins often affects the skin.
Fat-soluble vitamins:
Water-soluble vitamins:



Acrodermatitis enteropathica is an autosomal recessive inherited form of zinc deficiency that manifests in infancy. It presents with the clinical triad of dermatitis, alopecia and diarrhoea. Skin signs include:
See also Acrodermatitis enteropathica-like conditions.
Eruptive xanthomas are:



Dermatitis herpetiformis is associated with:
Skin signs of dermatitis herpetiformis include:



Inflammatory bowel disease (IBD) refers to ulcerative colitis and Crohn disease. There are similarities and differences in their cutaneous manifestations.
Aphthous ulcers are common in both forms of inflammatory bowel disease.



Erythema nodosum (EN) is the most common skin sign of Crohn disease (4-6%) or ulcerative colitis (3%).



Pyoderma gangrenosum (PG) affects 0.7% of patients with Crohn disease and 2% with ulcerative colitis.



Fissures and fistulae are common in Crohn disease (36%) and do not occur in ulcerative colitis.
Mucosal oedema affects 8–9% of patients with Crohn disease and is absent in ulcerative colitis.
Metastatic Crohn disease may cause cutaneous granulomatous plaques, nodules and ulcers.



Epidermolysis bullosa acquisita (EBA) is a rare immunobullous disorder sometimes associated with Crohn disease.



Cutaneous polyarteritis nodosa is a rare form of necrotising, small and medium-sized vasculitis.



Acute neutrophilic dermatosis, also known as Sweet syndrome, is an autoinflammatory disorder sometimes associated with inflammatory bowel disease. Features include:



Henoch-Schönlein purpura (HSP) is an immunoglobulin A-mediated, leukocytoclastic, small-vessel vasculitis.



Degos disease is small vessel angiopathy, thought to be due to dysregulation of interferon-alfa and the membranolytic attack complex. There are two variants: benign atrophic papulosis and malignant atrophic papulosis.



Hereditary haemorrhagic telangiectasia (HHT) is a hereditary, autosomal dominant, bleeding disorder.



Kaposi sarcoma (KS) is a human herpesvirus 8-associated tumour of endothelial cells.



Blue rubber bleb naevi are venous malformations of skin and gastrointestinal tract.



Pseudoxanthoma elasticum (PXE) is an inherited disease in which there are calcification and fragmentation of elastin fibres in the skin and internal organs.



Ehlers-Danlos syndrome (EDS) type IV is an inheritable connective tissue disease due to a defect in collagen synthesis.



Klippel–Trénaunay syndrome presents in infancy with a cutaneous capillary vascular malformation.



Bowel-associated dermatosis-arthritis syndrome (BADAS, bowel bypass syndrome) presents with recurrent and episodic flu-like symptoms, polyarthralgia and cutaneous lesions.



Hermansky-Pudlak syndrome is a form of tyrosine-positive oculocutaneous albinism with autosomal recessive inheritance.
Gardner syndrome is a variant of familial adenomatous polyposis with numerous adenomatous polyps and mucocutaneous findings, such as:

Hereditary nonpolyposis colorectal cancer, also known as Lynch syndrome, is the most common hereditary cancer.
Peutz-Jeghers syndrome is a hamartomatous polyposis syndrome with autosomal dominant inheritance.
Cowden syndrome, or multiple hamartoma syndrome, is characterised by skin lesions and polyposis coli.
Trichilemmomas are benign hamartomas of the outer sheath of hair follicles. They are:
Other skin lesions described in Cowden syndrome include:



The Bannayan-Riley-Ruvalcaba (BRR) syndrome is a rare germline mutation with hamartomatous polyposis, macrocephaly, and intellectual disability. Skin manifestations include:
Juvenile polyposis syndrome is a rare autosomal dominant disorder associated with hereditary haemorrhagic telangiectasia.
Neurofibromatosis is a common, autosomal dominant, a neurodermatosis characterised by:


Cronkhite-Canada syndrome is a sporadic syndrome that affects older adults. It presents with:
Acanthosis nigricans is associated with insulin resistance.



Tripe palm is associated with malignant acanthosis nigricans.


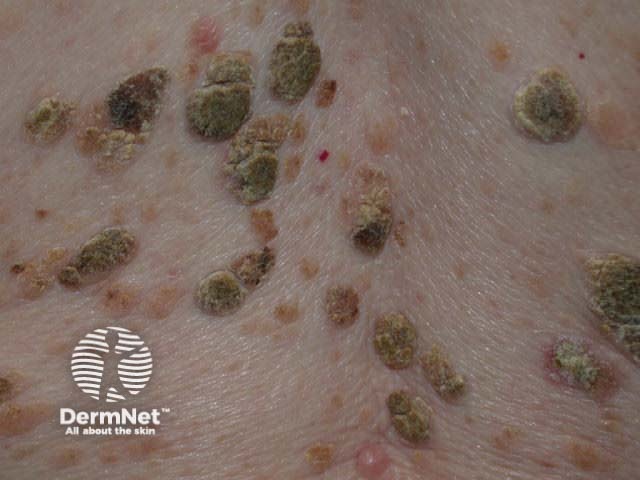
The acute onset of multiple, eruptive seborrhoeic keratosis is known as the sign of Leser-Trélat.

Acrokeratosis neoplastica is also known as Bazex syndrome and is different from Bazex-Dupré-Christol syndrome associated with basal cell carcinomas.
Glucagonoma is a rare, glucagon-secreting, pancreatic, alpha cell tumour.



Tylosis is an autosomal dominant form of focal, non-frictional and nonepidermolytic, palmoplantar keratoderma.



Plummer-Vinson syndrome is a rare triad of dysphagia, iron deficiency anaemia and oesophageal webs.

Extramammary Paget disease is an intraepithelial adenocarcinoma located in and around the anal verge, vulva, or male genitalia.

Carcinoid syndrome is the association of intestinal carcinoid with hepatic metastases.
Dermatomyositis is classified as an autoimmune disease. In older adults with dermatomyositis, 15–50% have an underlying malignancy of the gastrointestinal tract, pancreas, lung, breast, or ovaries, or non-Hodgkin lymphoma.



Paraneoplastic pemphigus (PNP) is a rare acantholytic, mucocutaneous blistering disease.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more