ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Prevention
Outcome
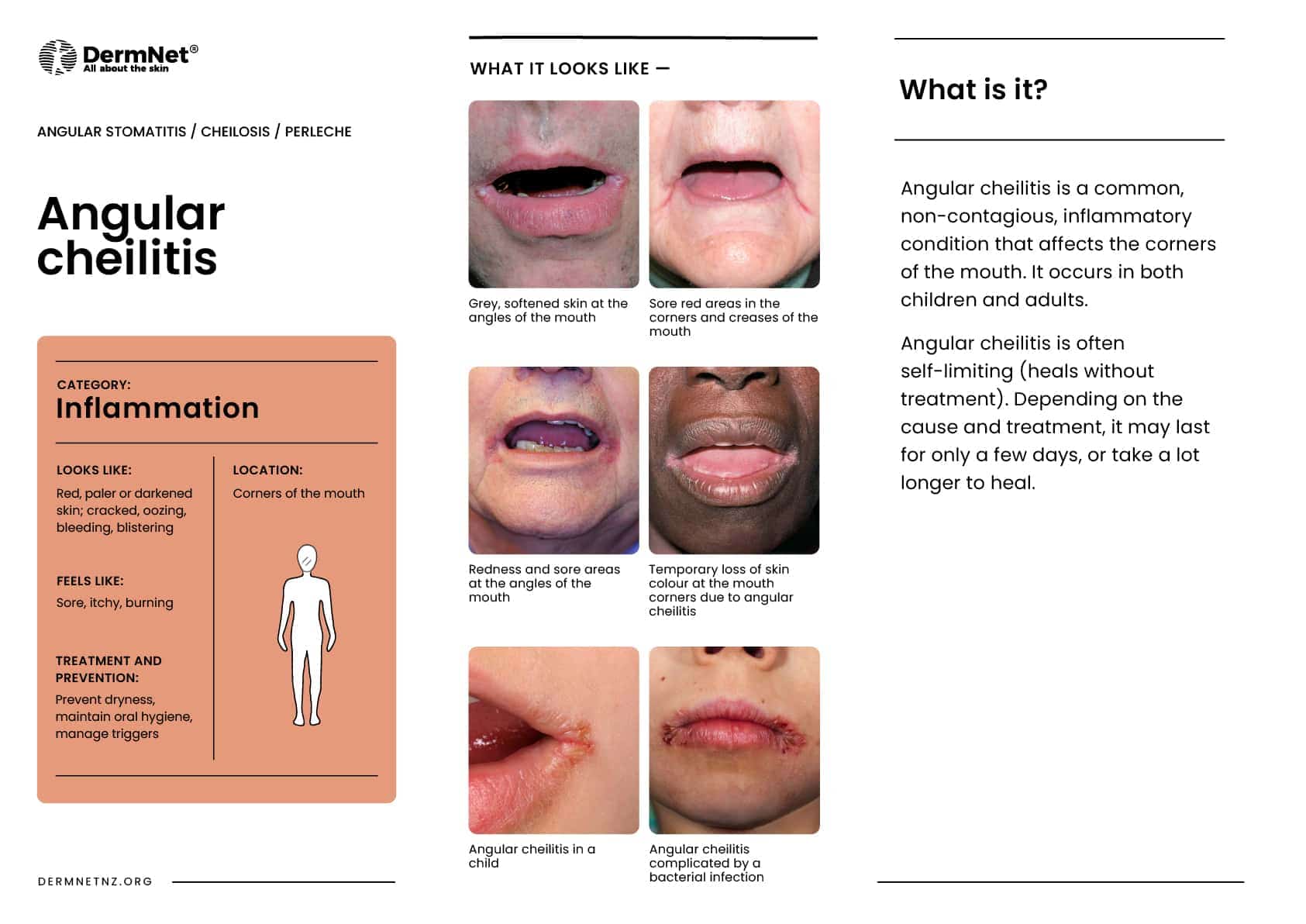
Angular cheilitis is a common, non-contagious, inflammatory condition affecting the corners of the mouth or oral commissures.
Depending on the underlying cause, it may last a few days or persist indefinitely. It is also called angular stomatitis, cheilosis, rhagades, or perleche (perlèche).





Angular cheilitis is common and can affect any child or adult. Those with poor health are especially susceptible.
Risk factors include:
It is made worse by licking the lips.
Angular cheilitis occurs at the angles of the mouth where two different types of skin lining meet and act as a hinge. The lining of the oral cavity (oral mucosa) meets with squamous epithelium (facial skin). As they are used often for eating, drinking, and talking, they are vulnerable to stress/trauma.
Angular cheilitis most commonly occurs due to prolonged exposure of the corners of the mouth to saliva and its digestive enzymes, resulting in eczematous cheilitis (a form of irritant contact dermatitis)
Angular cheilitis may result in the following symptoms and signs at the corners of the mouth:
It is usually bilateral and symmetrical, however, it can occur on one side. It may progress to more widespread impetigo or candidiasis (oral thrush) on the adjacent skin and elsewhere.
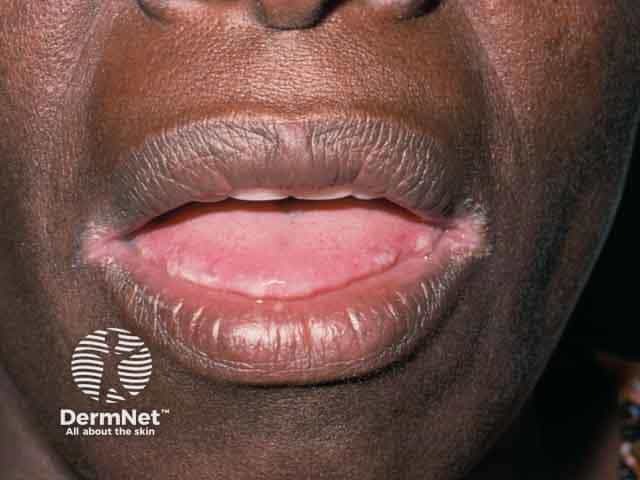
Angular cheilitis in dark skin may be more subtle in the initial stages, or the skin may appear pale rather than reddened. The pale areas of skin may also be surrounded by a darkened rim.
Angular cheilitis is diagnosed clinically based on history and examination.
The culture of swabs taken from the corners of the mouth may reveal:
Skin biopsy is not usually necessary.
In many cases, no treatment is needed and angular cheilitis resolves by itself.
Depending on the specific cause, oral and topical treatment options include:
In many cases angular cheilitis self-resolves, if not it is usually curable and rarely results in permanent scarring or pigmentation. Improvement is usually seen within the first few days of treatment and typically resolves by two weeks.
Repeat occurrences of angular cheilitis are common, especially in those with non-modifiable risk factors.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more