ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Outcome
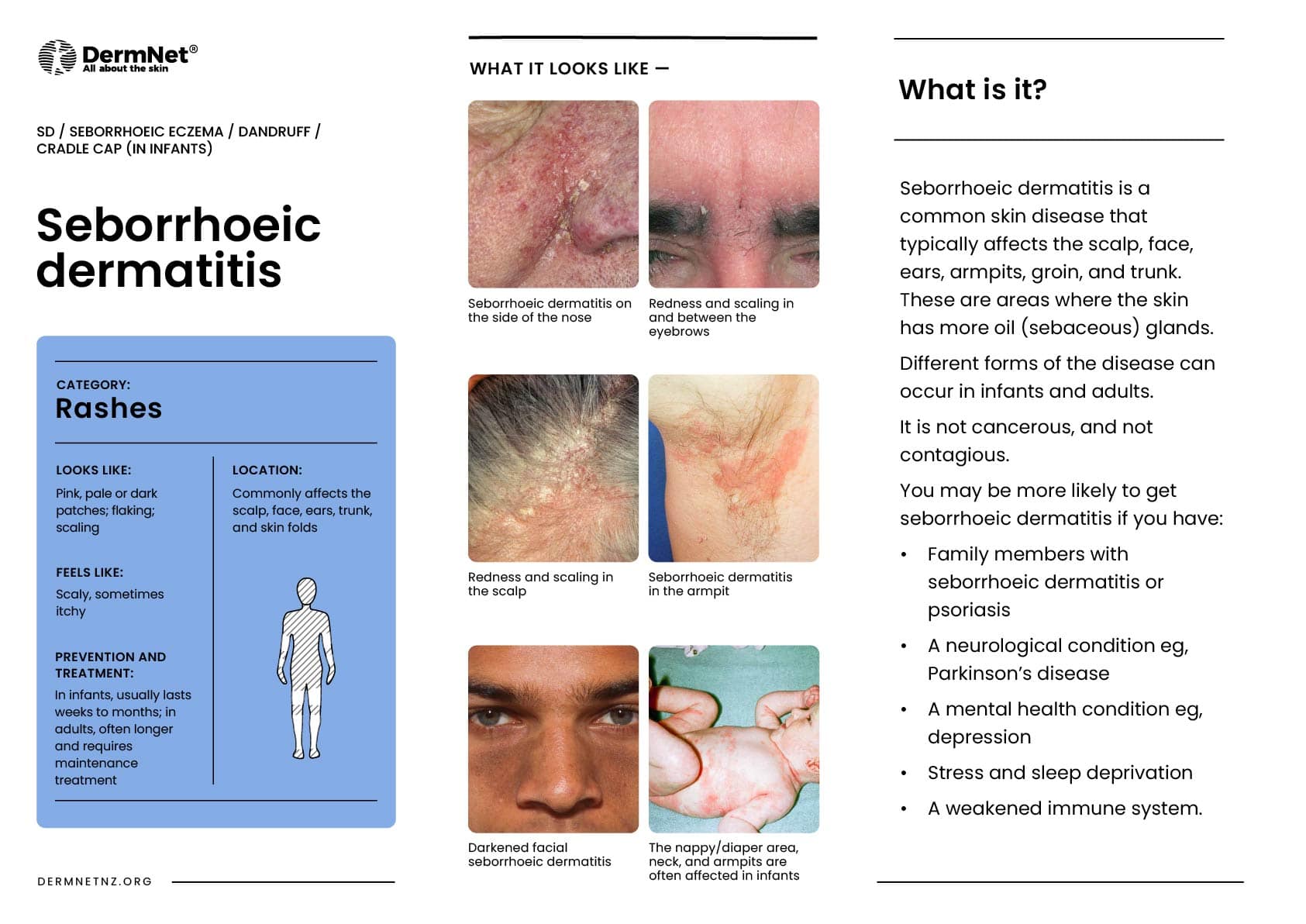
Seborrhoeic dermatitis is a common, chronic, or relapsing form of eczema/dermatitis that mainly affects the sebaceous gland-rich regions of the scalp, face, and trunk.
There are infantile and adult forms of seborrhoeic dermatitis. This benign inflammatory condition is sometimes associated with psoriasis and is known as sebopsoriasis. Seborrhoeic dermatitis is also known as seborrhoeic eczema (“seborrheic” in American English).
Dandruff (also called ‘pityriasis capitis’) is an uninflamed form of seborrhoeic dermatitis on the scalp. Dandruff presents as diffuse bran-like scaly patches within hair-bearing areas of the scalp without underlying erythema. Dandruff may be asymptomatic or mildly pruritic.






Seborrhoeic dermatitis is a common skin condition affecting 3% to 12% of the population.
It has a biphasic incidence occurring in infants and in adolescents and adults.
Infantile seborrhoeic dermatitis affects babies under the age of 3 months and usually resolves by 6-12 months of age.
Adult seborrhoeic dermatitis tends to begin in late adolescence. Prevalence is greatest in young adults and in older people. It is more common in males than in females.
Seborrhoeic dermatitis often occurs in otherwise healthy patients. However, the following factors are sometimes associated with severe adult seborrhoeic dermatitis:
The aetiology is not completely understood.
Several factors are associated with the condition e.g. hormone levels, fungal infections, nutritional deficits, neurogenic factors. Proliferation of Malassezia yeast genus is believed to play a role. The lipases and phospholipases produced by Malassezia, a saprophyte of normal skin, cleave free fatty acids from triglycerides present in sebum. This may induce inflammation. Differences in skin barrier lipid content and function may account for individual presentations.
Infantile seborrhoeic dermatitis causes cradle cap (diffuse, greasy scaling on the scalp). The rash may spread to affect armpit and groin folds (a type of napkin dermatitis).



Seborrheic dermatitis commonly affects areas of the skin with high sebum production, such as the scalp, nasolabial folds, glabella, eyebrows, beard, ears, retroauricular skin, sternum, and other skin folds.
Typical features include:
Extensive seborrheic dermatitis affecting the scalp, neck, and trunk is sometimes called pityriasiform seborrhoeide.
Seborrheic dermatitis is very common among patients of darker skin types. Studies have shown that it is among the five most common diagnoses observed in black patients.
People of darker skin may present with scaly hypopigmented macules and patches in typical areas of involvement. Arcuate or petal-like patches may be seen, termed petaloid seborrhoeic dermatitis.
Children of colour often do not experience the classic cradle cap appearance of seborrheic dermatitis, but instead have erythema, flaking, and hypopigmentation of the affected areas and folds of skin.

The diagnosis of seborrhoeic dermatitis is a clinical diagnosis based on the location, appearance, and behaviour of the lesions.
If the diagnosis is uncertain, a biopsy can be undertaken. This would typically show parakeratosis in the epidermis, plugged follicular ostia, and spongiosis in the case of seborrhoeic dermatitis. The dermis typically has a sparse, perivascular, lymphohistiocytic inflammatory infiltrate.
As Malassezia are a normal component of skin flora, their presence on microscopy of skin scrapings is not diagnostic.
For information on trichoscopic (dermoscopy) findings in seborrhoeic dermatitis, see trichoscopy of inflammatory conditions.
Treatment of seborrhoeic dermatitis often involves several of the following options.
In resistant cases in adults, oral itraconazole, tetracycline antibiotics, or phototherapy may be recommended. Low-dose oral isotretinoin has also been shown to be effective for severe or moderate disease.
Roflumilast 0.3% foam has had recent FDA approval for the use of seborrhoeic dermatitis in patients aged 9 years and older.
Regular washing of the scalp with baby shampoo or aqueous cream is followed by gentle brushing to clear the scales.
For more information, see infantile seborrhoeic dermatitis.
While seborrhoeic dermatitis may be self-limiting, it may take a long period of time to resolve. Cradle cap in infants usually takes a few weeks or months to disappear. In adults, the condition is frequently chronic and long-term maintenance treatment is often necessary.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more