
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction - hypogonadism Introduction - hypogonadism in males Causes Demographics Clinical features Skin changes Diagnosis Treatment and outcome
Hypogonadism is the inadequate function of the gonads (reproductive glands) leading to impaired production of germ cells and sex hormones.
Hypogonadism in males refers to diminished testicular function — a reduction in sperm production and in testosterone.
Hypogonadism is due to disruption to any section of the hypothalamic–pituitary–gonadal axis pathway (figure 1).
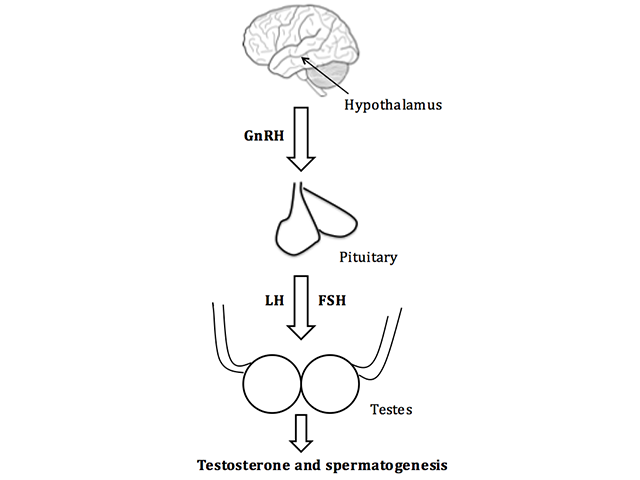
FSH; follicle-stimulating hormone, GnRH; gonadotropin-releasing hormone, LH; luteinising hormone
Both primary and secondary hypogonadism in males may be congenital or acquired.
Signs of congenital primary hypogonadism includes:
Acquired primary hypogonadism may be result of:
Congenital secondary hypogonadism results from isolated gonadotropin deficiency due to genetic mutations, such as Kallmann syndrome, Prader–Willi syndrome, and other similar conditions.
Acquired secondary hypogonadism may result from:
The clinical features of hypogonadism depend on the patient's age at presentation.
Hypogonadism at birth may be recognised by ambiguous genitalia (external genitals that are neither clearly male nor clearly female).
Hypogonadism pre-puberty may be diagnosed by the failure to undergo or complete puberty. The boy may have a young appearance, lack pubic hair, have small genitalia and testes, his voice may fail to break, and he may have difficulty in gaining muscle.
After the completion of puberty, the features of hypogonadism include decreased libido, erectile dysfunction, osteoporosis, depression, gynaecomastia, shrinking of the testes, and infertility. After some years of testosterone deficiency, decreased muscle mass and body hair may be evident.
Androgens are responsible for sebaceous gland growth and differentiation, hair growth, and epidermal barrier homeostasis [1].
Androgen deficiency results in:
The diagnosis of hypogonadism is based on observing typical clinical features in a man with low serum testosterone. The patient should be referred to a specialist.
Initial investigations should include measuring LH, FSH, and serum testosterone (usually taken in the morning, and repeated at least twice). If testosterone is low:
Further investigations should be directed at identifying the underlying cause.
Effective testosterone replacement in men with hypogonadism has been showed to maintain secondary sexual characteristics, increase libido, muscle strength, fat-free mass, and bone density [4].
Adverse effects of testosterone replacement include:
Testosterone should not be started in individuals with breast cancer, prostate cancer or an increased risk of prostate cancer, haematocrit above 50%, untreated obstructive sleep apnoea, severe lower urinary tract symptoms, or uncontrolled heart failure [4].
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more