
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Causes
Demographics
Clinical features
Complications
Skin changes
Diagnosis
Treatment
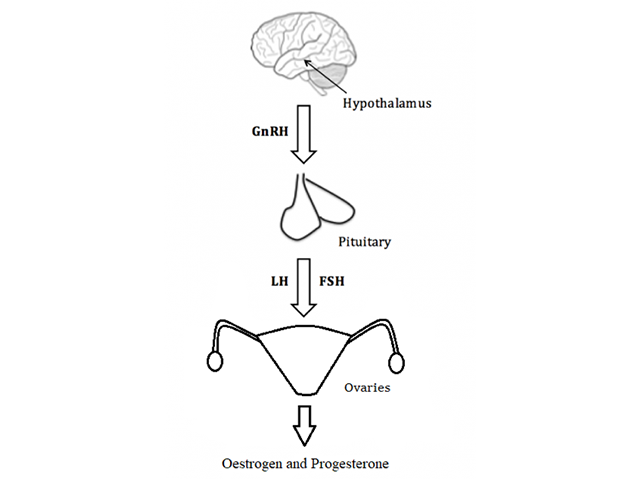
Hypogonadism in females describes the inadequate function of the ovaries, with impaired production of germ cells (eggs) and sex hormones (oestrogen and progesterone).
Hypogonadism in females is due to disruption of any section of the hypothalamic–pituitary–ovarian axis pathway (figure 1). In a correctly functioning hypothalamic–pituitary–ovarian axis pathway:
Primary ovarian insufficiency and secondary hypogonadism may be congenital or acquired [1,2].
The main mechanism for congenital primary ovarian deficiency remains unknown in the majority of cases. Some cases relate to:
The causes of acquired primary ovarian insufficiency include:
Congenital secondary hypogonadism is gonadotrophin deficiency due to a genetic mutation, such as in Kallmann syndrome.
Acquired secondary hypogonadism can be due to damage to the pituitary/hypothalamus. Causes of acquired secondary hypogonadism can include:
Gonadotropins can be suppressed by:
The clinical features of hypogonadism depend on the age at presentation [3].
Symptoms of low oestrogen levels are rarely present in hypogonadism pre-puberty. The presenting features are absent pubertal development (reduced growth and absence of pubic hair) and primary amenorrhoea (absence of menarche).
After the completion of puberty, the features of hypogonadism include:
The long-term risks of oestrogen deficiency include an increased risk of osteoporosis and cardiovascular disease. The risk is greater with a younger age of onset. In contrast, the risk of breast cancer may be slightly reduced.
Oestrogen has a key role in maintaining skin health. Oestrogen helps maintain skin thickness and collagen levels, skin elasticity, and moisture. It is also thought to play a role in wound healing [4].
Low oestrogen levels are associated with:
Skin changes may also reflect the underlying cause of hypogonadism; for example, hyperpigmentation may be a sign of an autoimmune disease.
If hypogonadism is suspected following a detailed history and examination, the following investigation pathway can be followed.
Treatment of hypogonadism is directed at the underlying pathology where possible, helping the woman become fertile if desired, and preventing the long-term complications of hypoestrogenism (ie, osteoporosis, increased cardiovascular disease, and urogenital atrophy).
As a general rule, women of reproductive age with hypoestrogenism should receive hormone replacement therapy. Specialist input should be sought, as there are potential significant complications of hormone therapy, such as:
Post-menopause, hormone replacement therapy is indicated for significant symptoms.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more