
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Causes
Clinical features
Cutaneous features
Diagnosis
Complications
Differential diagnoses
Management
Prader–Willi syndrome is the most common genetic cause of obesity. It was first described in 1887 by John Langdon Down, 70 years before Prader et al in 1956. It is also known as Prader–Labhart–Willi syndrome.

* Credit: Museo Nacional del Prado.
Prader–Willi syndrome is reported to occur approximately once in 25,000 live births, but it is likely to be more common due to a failure to diagnose the condition early.
Prader–Willi syndrome has autosomal dominant inheritance, (is inherited from one affected parent) and affects both sexes and all races. However, most cases are sporadic.
Prader–Willi syndrome results from the lack of expression of the PWC region of chromosome 15. The genes for Prader–Willi syndrome are normally expressed only on the chromosome inherited from the father, and the copy of chromosome 15 inherited from the mother is switched off.
Three mechanisms are involved.
Angelman syndrome is a clinically distinct disorder that results from a maternally derived imprinting defect mapped to the same chromosome as Prader–Willi syndrome.
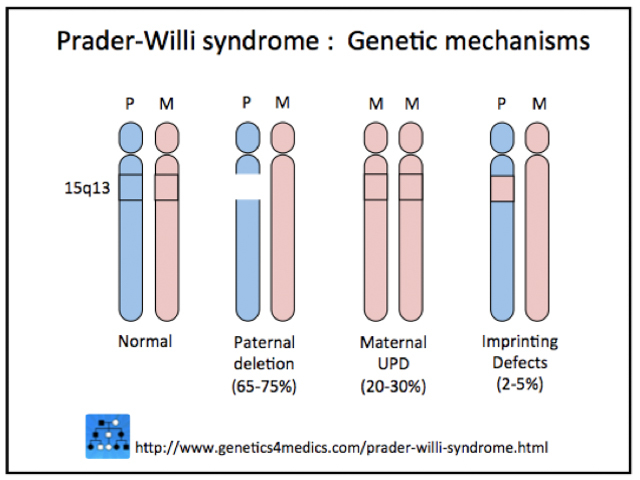
*Image courtesy Genetics 4 Medics.
The clinical features of Prader–Willi syndrome depend on the age of the individual.

Skin picking is very common and is the most typical cutaneous feature of Prader–Willi syndrome. Lesions are present at all stages of the evolution of the syndrome. Signs include scratch marks, bleeding, bacterial skin infection, scabs, scarring, and secondary milia — especially on the backs of the hands and forearms.
Other cutaneous features may include:
There are also single case reports of urticaria pigmentosa, extremely dry skin, seborrhoeic dermatitis, and pseudo-Kaposi sarcoma.
Features of Prader–Willi syndrome can include:
Features of Prader–Willi syndrome can include:



The following diagnostic criteria may be used to diagnose Prader–Willi syndrome.
Each of the following criteria scores 1 point:
Each of the following criteria scores 1 point:
Genetic studies are the most accurate way to diagnose Prader–Willi syndrome. Such studies should be considered in any floppy newborn baby requiring tube feeding. All three mechanisms for the syndrome should be looked for sequentially, starting with the paternal deletion.
X-rays should be undertaken during childhood to identify skeletal problems, as these can be masked by obesity.
In adult life, dermatological problems requiring treatment are a major health issue, with erysipelas being a common reason for hospital admission.
Medical complications of Prader–Willi syndrome include:
The differential diagnosis of Prader–Willi syndrome includes other causes of obesity and failure to thrive in infancy and childhood.
One Prader–Willi-like syndrome to be considered is 6q16 deletion syndrome, which is due to proximal deletions of the long arm of chromosome 6. Its main features are:
Genetic counselling is recommended for future pregnancies and family members. Special care may be needed with general anaesthesia for individuals with Prader–Willi syndrome. Treatments deal with medical and surgical complications and associations as they arise and are related to the affected individual's age.
Hospital admissions may be required for:
Hospital admission may be required for:
Medications used by adults with Prader–Willi syndrome include psychotropics, laxatives, skin products, and treatments for diabetes.
Respiratory infections are a major health issue in older adults.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more