Author: Hon A/Prof Amanda Oakley, Dermatologist, Hamilton, New Zealand, 1998. Revised and updated August 2015. Updated by Janet Dennis, November 2018. Technical Editor: Mary Elaine Luther, Medical Student, Ross University, Barbados. DermNet Editor in Chief: Adjunct A/Prof Amanda Oakley, Dermatologist, Hamilton, New Zealand. Copy edited by Gus Mitchell. January 2020.
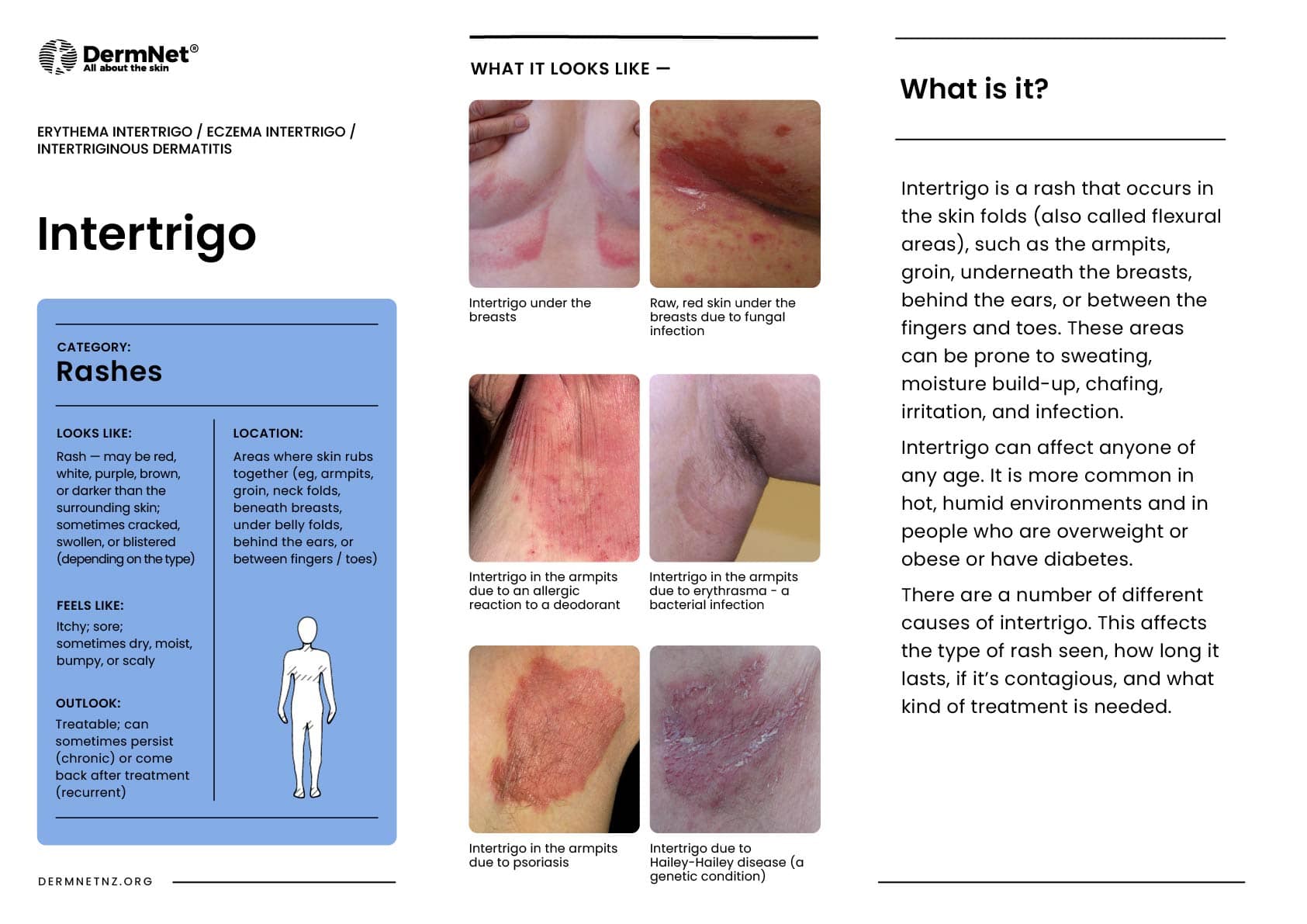
Intertrigo describes a rash in the flexures, such as behind the ears, in the folds of the neck, under the arms, under a protruding abdomen, in the groin, between the buttocks, in the finger webs, or in the toe spaces. Although intertrigo can affect only one skin fold, intertrigo commonly involves multiple sites. Intertrigo is a sign of inflammation or infection.
Who gets intertrigo?
Intertrigo can affect males or females of any age. Intertrigo is particularly common in people who are overweight or obese (see metabolic syndrome).
In infants, napkin dermatitis is a type of intertrigo that primarily occurs due to skin exposure to sweat, urine, and faeces in the diaper area.
Toe-web intertrigo is associated with closed-toe or tight-fitting shoes. Lymphoedema is also a cause for toe-web intertrigo.
What are the clinical features of intertrigo?
Intertrigo can be acute (recent onset), relapsing (recurrent), or chronic (present for more than six weeks). The exact appearance and behaviour depend on the underlying cause(s).
The skin affected by intertrigo is inflamed, reddened, and uncomfortable. The affected skin can become moist and macerated, leading to fissuring (cracks) and peeling.
Intertrigo is due to genetic and environmental factors.
Flexural skin has a relatively high surface temperature.
Moisture from insensible water loss and sweating cannot evaporate due to occlusion.
Friction from the movement of adjacent skin results in chafing.
Intertrigo occurs more easily in environments that are hot and humid.
Diabetes, alcohol, and smoking increase the likelihood of intertrigo, especially the infectious form.
The microbiome (microorganisms normally resident on the skin) on flexural skin includes Corynebacterium, other bacteria, and yeasts. Microbiome overgrowth in warm moist environments can cause intertrigo.
Intertrigo is classified into infectious and inflammatory origins, but they often overlap.
Infections tend to be unilateral and asymmetrical.
Atopic dermatitis is usually bilateral and symmetrical, affecting the flexures of the neck, knees and elbows.
Other inflammatory disorders also tend to be symmetrical affecting the armpits, groins, under the breasts, and the abdominal folds.
A skin biopsy may be performed for histopathology if the skin condition is unusual or fails to respond to treatment.
What is the treatment for intertrigo?
Treatment depends on the underlying cause if identified, and on which micro-organisms are present in the rash. Combinations are common.
Zinc oxide paste can be used for napkin dermatitis or incontinence-associated irritant contact dermatitis.
Physical exertion should be followed by bathing and completely drying skin flexures. A hairdryer on cool setting is an effective approach for drying underarms and breasts.
Sweating can be reduced with an antiperspirantcream or powder.
Inflammatory skin diseases are often treated with low potency topical steroidcreams such as hydrocortisone. More potent steroids are best avoided in the flexures because they can cause skin thinning, resulting in stretch marks (striae atrophicae) and rarely, ulcers.Calcineurin inhibitors such as tacrolimus ointment or pimecrolimus cream are also effective in skin folds.
References
Janniger CK, Schwartz RA, Szepietowski JC, Reich A. Intertrigo and common secondary skin infections. Am Fam Physician 2005; 1; 72: 833–8. Journal
Tüzün Y, Wolf R, Baglam S, Engin B. Diaper (napkin) dermatitis: a fold (intertriginous) dermatosis. Clin Dermatol 2015; 33: 477–82. PubMed
De Britto LJ, Yuvaraj J, Kamaraj P, Poopathy S, Vijayalakshmi G. Risk factors for chronic intertrigo of the lymphedema leg in southern India: a case-control study. Int J Low Extrem Wounds 2015; 14: 377–83. doi: 10.1177/1534734615604289.PubMed
Martín EG, Sánchez RM, Herrera AE, Umbert MP. Topical tacrolimus for the treatment of psoriasis on the face, genitalia, intertriginous areas and corporal plaques. J Drugs Dermatol 2006; 5: 334–6. PubMed
Weidner T, Tittelbach J, Illing T, Elsner P. Gram‐negative bacterial toe web infection–a systematic review. J Eur Acad Dermatol Venereol 2018; 32: 39–47. PubMed