Author: Dr Ahmed Sadek, Dermatologist, Cairo Hospital for Dermatology & Venereology (Al-Haud Al-Marsoud), Egypt (2022)
Contributors: Dr Dalia Hossam, Dr Radwa Magdy, Dr Nehal Saied, Dr Noha Hashem, Dr Safaa Yehia Negm, Dr Moshera Saied El Bahrawy, Dr Amira Ragab, Dr Amal Wagih, Dr Haidy El-Hussieny, Dr Mona Ragib, Dr Hala Amer (2022)
Many scalp and hair disorders present with focal hairless patches which require meticulous examination to differentiate between cicatricial (scaring) and noncicatricial (non-scarring) alopecia and to identify their exact cause. Trichoscopy can be used as a non-invasive tool for rapid diagnosis of different types of alopecia.
Tinea capitis is a superficial fungal infection of the scalp commonly affecting children, however it may present in immunosuppressed adults. The disease is primarily caused by dermatophytes, Trichophyton and Microsporum genera, that cause endothrix or ectothrix type hair shaft infection respectively.
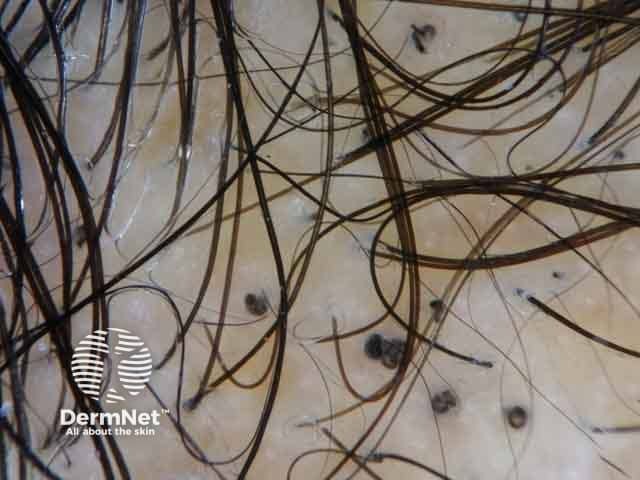
The clinical presentation is typically of a single or multiple patches of hair loss, sometimes with a black dot pattern, that may be accompanied by inflammation, scaling, pustules, and itching.
Trichoscopic features
Specific features:
Comma hairs
Corkscrew hairs.
Comma and corkscrew hairs represent the bending of the affected hair shafts due to the invasion with fungal hyphae.
Dermoscopic image of tinea capitis presenting with comma hairs
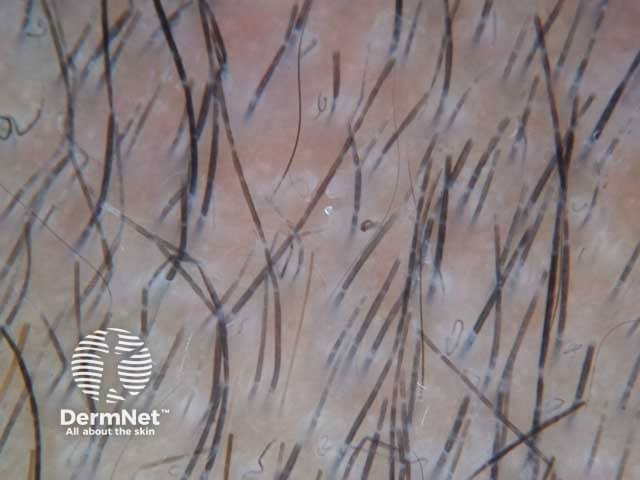
Dermoscopic image of tinea capitis presenting with corkscrew hairs
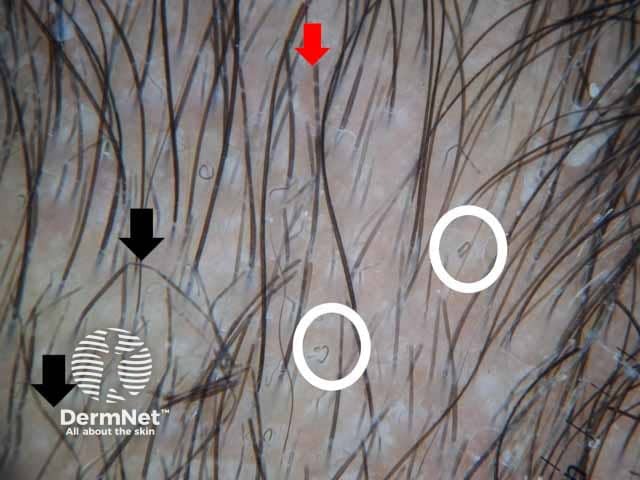
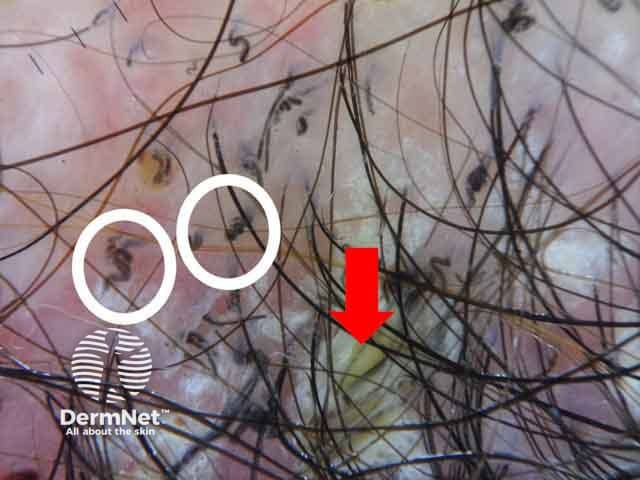
Dermoscopic image showing comma hair (white circles) zigzag hair (black arrows) and morse-code hair (red arrows) denoting tinea capitis (TC-patient1)
Other features:
Heterogeneous black dots
Broken and dystrophic hairs
Zigzag hairs
Morse code (barcode) hairs are reported: clue of ectothrix infection by Microsporum canis
White or yellow greasy scales
Erythematousperifollicular skin, V-shaped hair, crusts, and follicular pustules are observed in inflammatory types
Follicular keratosis in non-inflammatory type
Dermoscopic image of tinea capitis showing zigzag hairs; focal weakening of the hair shaft in a male child
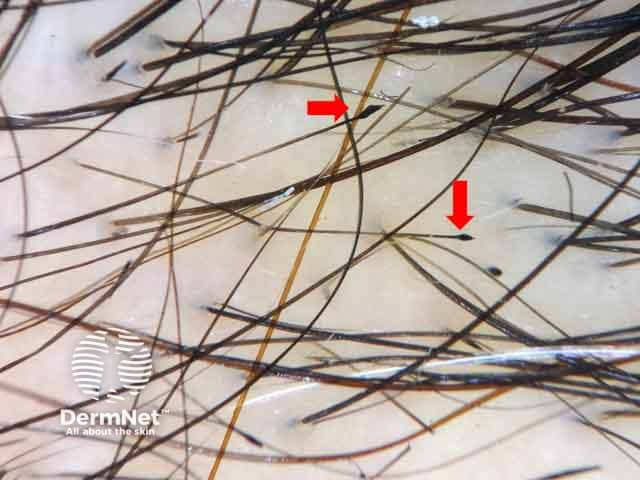
Dermoscopic image of tinea capitis showing morse code–like hair; interrupted hairs with multiple bands along the hair shaft in a female child.
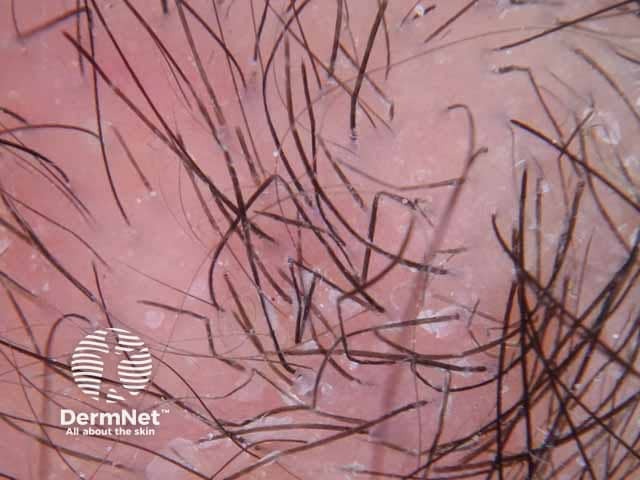
Dermoscopic image of corkscrew hairs (white circles) with yellowish greasy scales (red arrows) denoting tinea capitis. (TC-patient2)
Trichotillomania
Trichotillomania is a body-focused repetitive behaviour disorder. Sufferers may derive pleasure, gratification, or relief when pulling out their hair. It presents with irregular patches of alopecia, with hairs of variable length commonly affecting the vertex or parietal scalp.
Trichoscopic features
Specific features:
Hairs broken at different lengths
Irregular coiled hairs
Flame figures frequently in early childhood patients
V-sign
Hair powder.
Dermoscopic image of trichotillomania showing flame figures; hair remnants of recently pulled hairs
Trichotillomania showing V-sign that represents two hair shafts emerging from the same follicle and cut at the same level
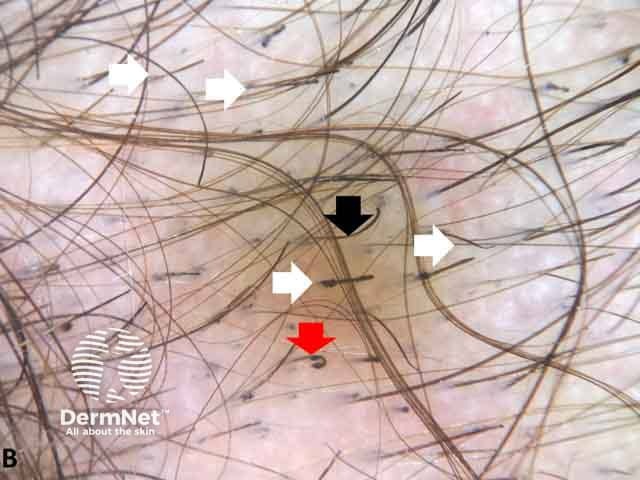
Dermoscopic image showing hair cut at different levels (white arrows), hook hair (black arrows) and flame figures (red arrows) denoting trichotillomania (TTM-patient1)
Other features:
Heterogeneous black dots
Hook hairs
Trichoptilosis
Extravasated blood
Tulip hairs
Upright regrowing hairs
Yellow dots with cadeverized hair in the center
Micro–exclamation mark hairs are sometimes described
Pluck-out sign is described in beard trichotillomania as presence of hemorrhages around the hair follicles
Less common: comma hairs, crusts, scales, dirty dots, and honeycomb pigment network.
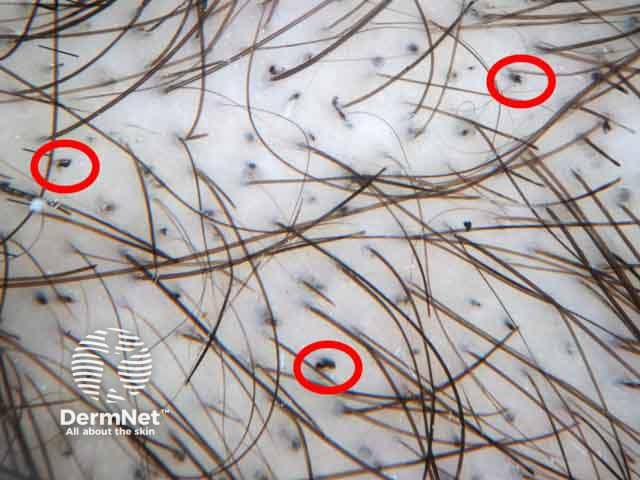
Trichotillomania showing black dots; follicular openings with remnants of pigmented hairs broken at scalp level
Trichotillomania showing hook hair (red arrow)
Dermoscopic image of trichotillomania showing tulip hair; hair shaft with darker distal end
Temporal triangular alopecia is a non-scarring, circumscribed alopecia is often located unilaterally in the frontotemporal region during early childhood and remains stationary throughout life.
Trichoscopic features
Normal follicular openings.
Vellus hairs of variable length and white hairs are reported.
Central tuft of terminal hairs may be present in some patients.
Absent characteristic features suggestive of other disorders.
Clinical image of a male patient with patchy hair loss in the temporal area. (TTA-patient1)
Normal follicular openings with vellus hairs coveirng an area of triangular temporal alopecia. (TTA-patient1)
Bibliography
Abraham LS, Torres FN, Azulay-Abulafia L. Dermoscopic clues to distinguish trichotillomania from patchy alopecia areata. An Bras Dermatol. 2010;85(5):723–6. doi:10.1590/s0365-05962010000500022. Journal
Aqil N, BayBay H, Moustaide K, Douhi Z, Elloudi S, Mernissi FZ. A prospective study of tinea capitis in children: making the diagnosis easier with a dermoscope. J Med Case Rep. 2018;12(1):383. Published 2018 Dec 28. doi:10.1186/s13256-018-1914-6. Journal
Cutrone M, Grimalt R. The Dermoscopic "Pluck Out Sign" for Beard Trichotillomania. Skin Appendage Disord. 2018;4(1):15–17. doi:10.1159/000477588. Journal
Hughes R, Chiaverini C, Bahadoran P, Lacour JP. Corkscrew hair: a new dermoscopic sign for diagnosis of tinea capitis in black children. Arch Dermatol. 2011;147(3):355–6. doi:10.1001/archdermatol.2011.31. Journal
Rakowska A, Slowinska M, Olszewska M, Rudnicka L. New trichoscopy findings in trichotillomania: flame hairs, V-sign, hook hairs, hair powder, tulip hairs. Acta Derm Venereol. 2014;94(3):303–6. doi:10.2340/00015555-1674 Journal
Ross EK, Vincenzi C, Tosti A. Videodermoscopy in the evaluation of hair and scalp disorders. J Am Acad Dermatol. 2006;55(5):799–806. doi:10.1016/j.jaad.2006.04.058. Abstract
Shim WH, Jwa SW, Song M, et al. Dermoscopic approach to a small round to oval hairless patch on the scalp. Ann Dermatol. 2014;26(2):214-220. doi:10.5021/ad.2014.26.2.214. Journal
Slowinska M, Rudnicka L, Schwartz RA, et al. Comma hairs: a dermatoscopic marker for tinea capitis: a rapid diagnostic method. J Am Acad Dermatol. 2008;59(5 Suppl):S77-S79. doi:10.1016/j.jaad.2008.07.009. Abstract