
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Androgenetic alopecia
Alopecia areata
Diffuse alopecia
Telogen effluvium
Anagen effluvium
Tractional alopecia
Generalised noncicatricial hair loss is a non-scarring, potentially reversible type of hair loss.
Main causes of generalised noncicatricial alopecia:
Androgenetic alopecia is one of the most common causes of hair loss worldwide. A progressive decline in the diameter, length, and pigmentation of the hair shaft with characteristic distribution is observed.
This occurs when androgens induce miniaturisation through shortening of the anagen duration and prolongation of the telogen phase in genetically susceptible hair follicles. It is characterised by frontotemporal recessions and loss of hair over the vertex. Complete loss of hair can occur except at the lateral and posterior margins of the scalp.
This condition is a multifactorial disorder in which different genes, increased dihydrotestosterone production in the skin, lack of intracutaneous synthesised estrogens, and abnormalities in prolactin-mediated signalling may contribute to the pathogenesis. It is characterised by diffuse thinning without frontal hairline recession.
Assessment of the scalp should be undertaken in the midline of the frontal area at a point 2cm from the frontal hair and compared with the occipital area of scalp.
Diagnostic signs:
Other signs:

Alopecia areata is a chronic inflammatory T-cell mediated autoimmune disease targeting the hair follicles of the scalp and body. Clinical subtypes include:
Associated nail changes include fine pitting, longitudinal ridges, and thinning may be observed.
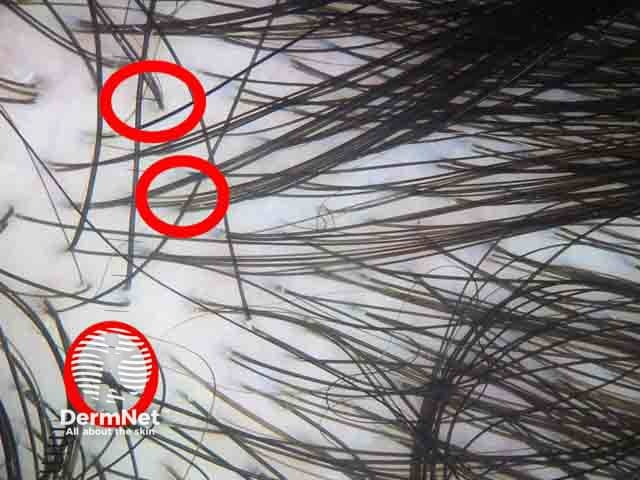
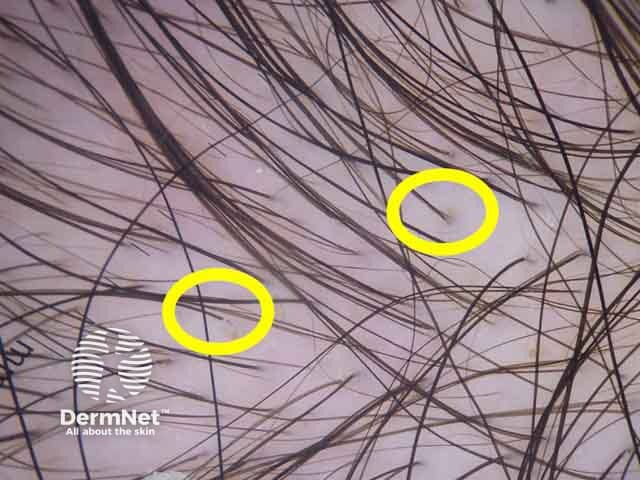
Trichoscopic features of alopecia areata differ according to activity, severity, and duration of disease.
Signs of active disease:
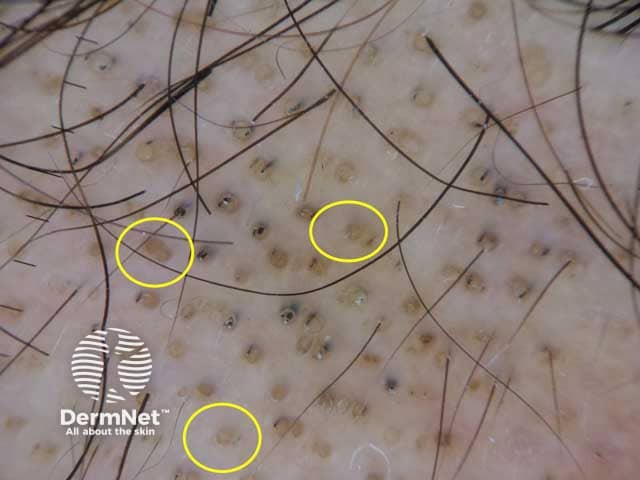
Signs of severe long-standing disease:
Other signs:



Diffuse alopecia (alopecia areata incognito) is a variant of alopecia areata, characterised by diffuse hair thinning with an absence of the typical patches of alopecia. It is more evident in the occipital and parietal regions and usually affects adult females. The diagnosis is confirmed only by histopathology as trichoscopic features are not specific.
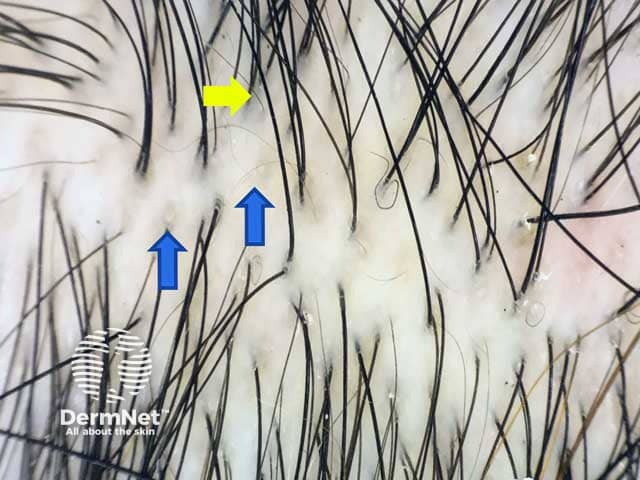
Telogen effluvium is characterised by excessive shedding of hair in the telogen phase. Alteration of the normal hair cycle occurs as a result of psychological and emotional stress. In scalp hair, more than 20% telogen hairs is considered diagnostic. Clinically, telogen effluvium may be:
Often occurs 3 months after the triggering event such as high fever, surgical trauma, sudden starvation, and haemorrhage. However, in one-third of patients with telogen effluvium, no triggering event is identified.
Hair shedding persists for more than 6 months. It occurs due to chronic primary telogen effluvium, or due to underlying medical disorder, eg. thyroid disease, iron deficiency anaemia, acrodermatitis enteropathica, and malnutrition.
The role of trichoscopy in diagnosis of telogen effluvium is limited. Trichoscopic features are not specific and include:

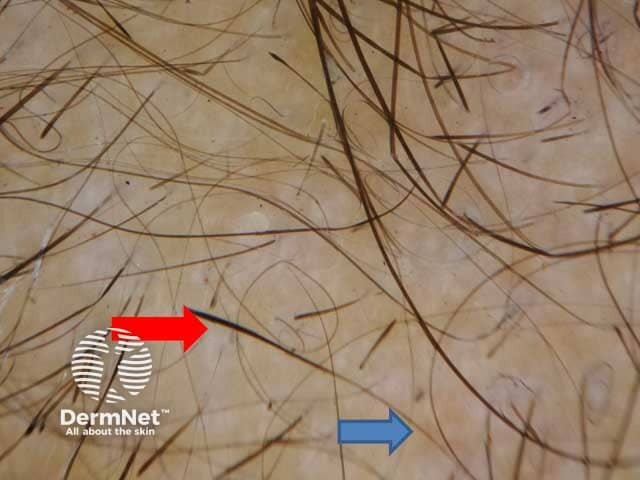
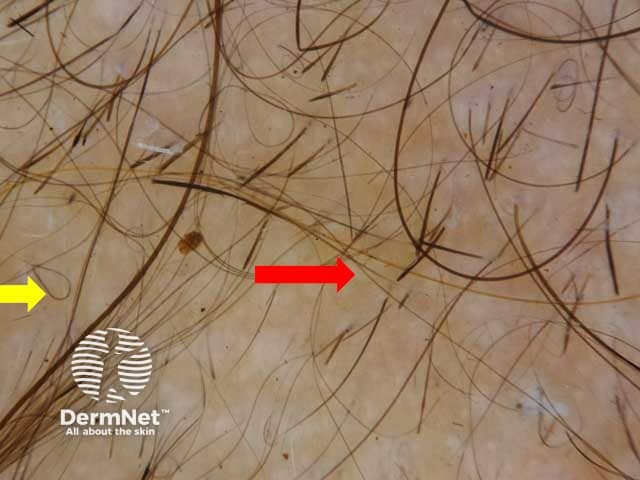
Anagen effluvium is a diffuse loss of hair in the anagen phase. It occurs in patients undergoing chemotherapy, or radiation therapy due to alteration of the hair cycle.
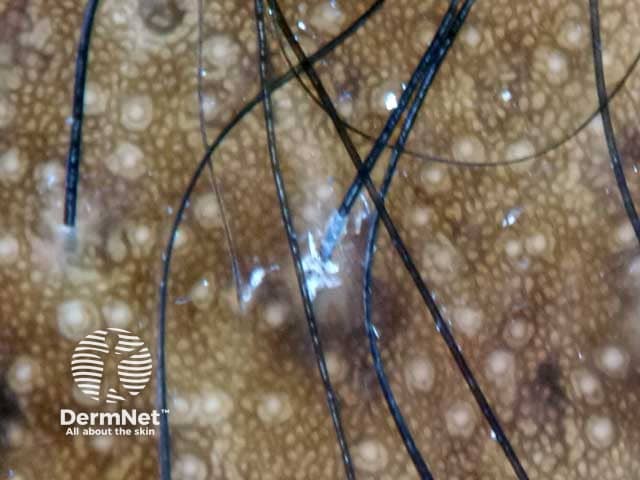
Tractional alopecia is a form of traumatic hair loss, due to severe tension on scalp hairs. Frontal and tempro-parietal areas are most frequently affected. It may be marginal or non-marginal. The marginal type shows mild perifollicular erythema in areas of traction. This type is common in children and women of African descent. Non-marginal type is quite common in neonates affecting the occipital area within the first weeks of life.
The main trichoscopic clues for diagnosis are:

For general information on features found using trichoscopy, see trichoscopy (an overview).
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more