Authors: Dr Charlotte Foster, Anatomical Pathology Registrar, Tauranga, New Zealand; Dr Ben Tallon, Consultant Dermatopathologist, Tauranga, New Zealand. Copy edited by Gus Mitchell. September 2021
Seborrhoeic keratosis is a benignacanthoma comprised of epidermalkeratinocytes. Clinically it presents as a sharply demarcatedwartyplaque with a ‘stuck-on’ appearance and greasy texture.
What is the histology of seborrhoeic keratosis?
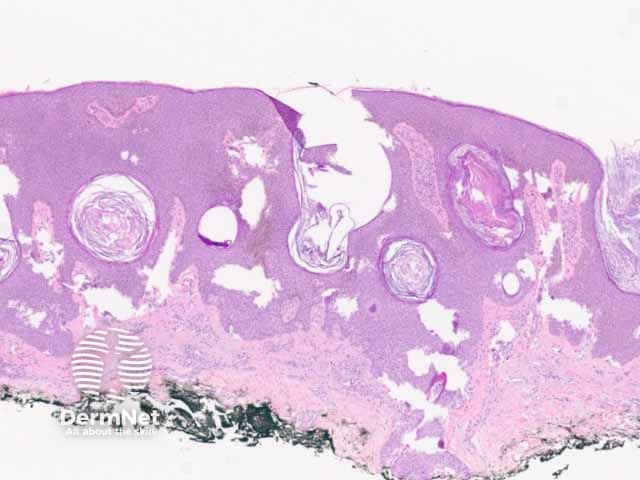
Seborrhoeickeratosis is a well-demarcated exophytic, flat or, less commonly, endophytic lesion composed of a proliferation of epidermal keratinocytes. Seborrhoeic keratosis can be recognised by a papillomatous architecture, acanthosis, hyperkeratosis, and horncysts. The hyperkeratosis produces a characteristic loose lamellar stratum corneum.Squamous eddies may be present if particularly acanthotic.
There are multiple distinct histological patterns:
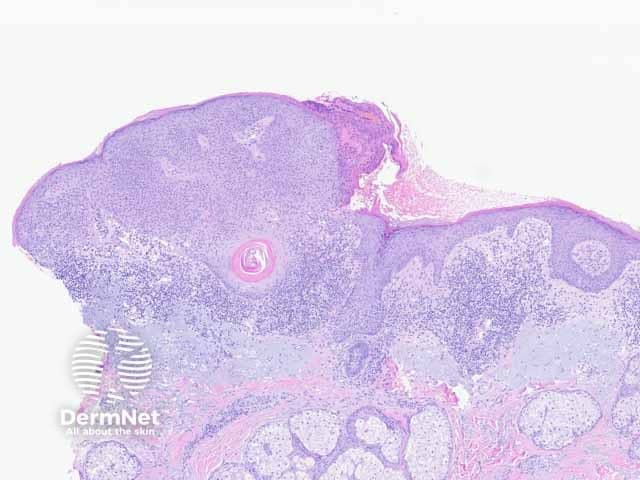
Regular acanthotic (Figure 1)
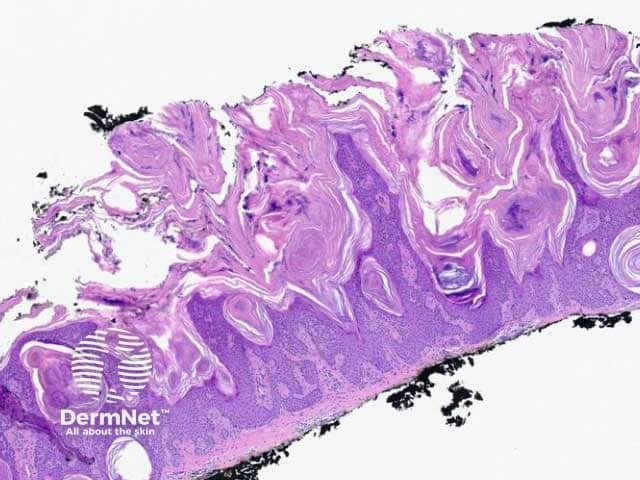
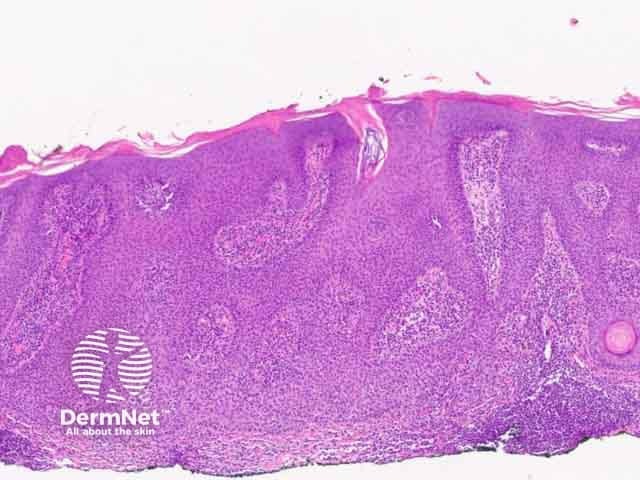
Keratotic papillomatous (Figure 2)
Exaggerated hyperkeratosis and papillomatosis
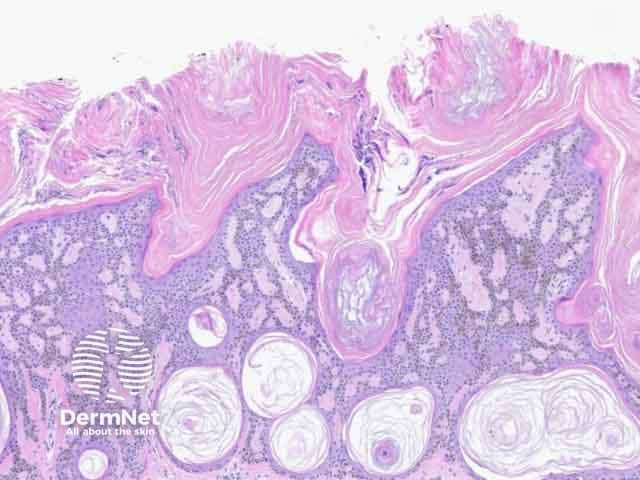
Reticulated adenoid (Figure 3)
Thinned rete ridges which articulate
Small horn cysts
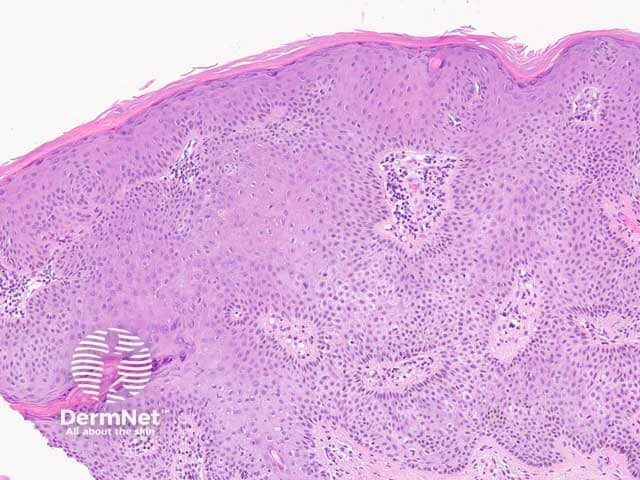
Clonal (Figure 4)
Nests of clear keratinocytes in the epidermis
Irritated (Figure 5)
Scalecrust, focal squamous eddies
Underlying lichenoidinflammation
Pigmented (Figure 3)
Increased epidermal pigment
Dermalmelanophages
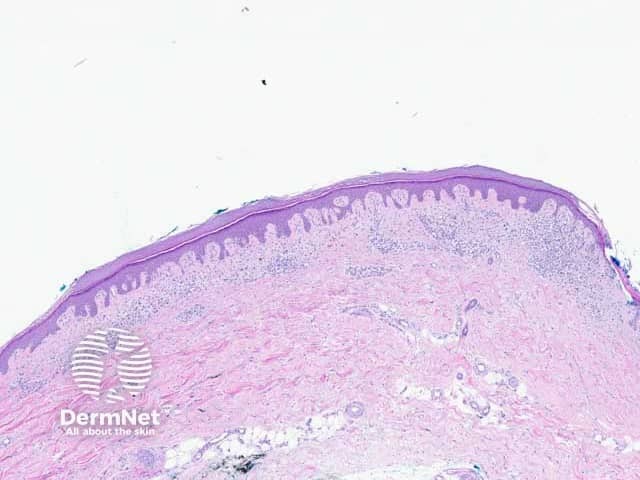
Macular (Figure 6)
No horn cysts
May be difficult to distinguish from solar lentigo
Overlap with additional features
Pigmented, irritated, or inflamed (Figure 7)
Histological patterns of seborrhoeic keratosis
Figure 2: keratotic papillomatous pattern
Figure 3: reticulated adenoid pattern
Figure 4: clonal pattern
Figure 5: irritated pattern
Figure 6: macular pattern
Figure 7: inflamed pattern
What is the differential diagnosis of seborrhoeic keratosis pathology?
Verruca vulgaris: The keratotic papillomatous variant of seborrheic keratosis is histologically very similar to verruca vulgaris. However, verruca vulgaris shows koilocytes and inward bending rete. Horn cysts are not usually seen in verruca vulgaris [see Verruca vulgaris pathology].
Epidermal naevus: While the histological features may be similar, the history will be of a longstanding lesion typically appearing at birth or in early childhood [see Epidermal naevus pathology].
Confluent and reticulated papillomatosis: This presents as a netlike hyperpigmentederuption of papules and plaques so it is clinically quite distinct from a seborrheic keratosis, although the histology can be similar.
Bibliography
Elston D, Ferringer T. Dermatopathology, 3rd edn, Elsevier, 2018
Groesser L, Herschberger E, Landthaler M, Hafner C. FGFR3, PIK3CA and RAS mutations in benign lichenoid keratosis. Br J Dermatol. 2012;166(4):784–8. doi:10.1111/j.1365-2133.2011.10788.x. PubMed
Calonje E, Brenn T, Lazar A, Billings S. McKee’s Pathology of the Skin, 5th edn, Elsevier, 2018.
Minagawa A. Dermoscopy-pathology relationship in seborrheic keratosis. J Dermatol. 2017;44(5):518–24. doi:10.1111/1346-8138.13657. PubMed