Pityriasiform seborrhoeide is an unusual variant of seborrhoeic dermatitis. Seborrhoeicdermatitis is a common flaky skin form of dermatitis that mainly affects scalp and skin folds around the ears and face. Pityriasiform seborrhoeide is more widespread and inflammatory than usual seborrhoeic dermatitis.
What are the features of pityriasiform seborrhoeide?
Pityriasiform seborrhoeide is characterised by:
Generalised light pink scalyrash, similar on both sides of the body
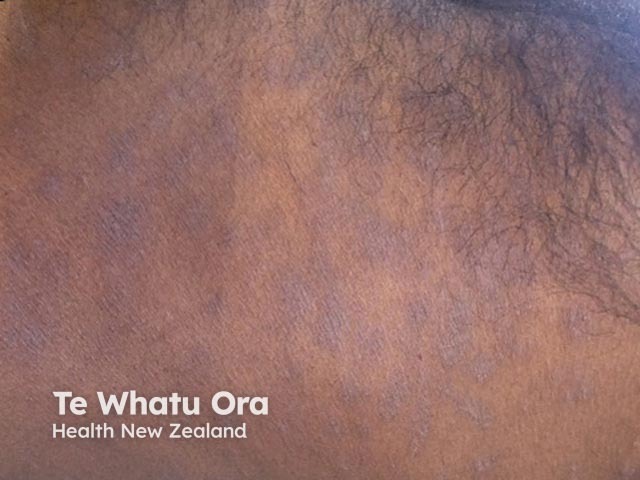
In darker skins, patches may be pigmented
Tends to be most severe on scalp, ears, face, neck, trunk but may spread to limbs
Lesions form poorly-defined oval flaky patches
May become eczematised, with weeping or oozing areas
Chronic eczematised areas may become lichenified (thickened, with increased skin markings)
Itch can be absent, minimal or severe (if eczematised)
Pityriasiform seborrhoeide
Pityriasiform seborrhoeide
Pityriasiform seborrhoeide
Pityriasiform seborrhoeide
Pityriasiform seborrhoeide
Pityriasiform seborrhoeide
What causes pityriasiform seborrhoeide?
Pityriasiform seborrhoeide is thought to be a hypersensitivity dermatitis related to the presence of common Malassezia yeasts on the skin surface.
It is not infectious, and generally does not recur once it has been effectively treated.
How is pityriasiform seborrhoeide diagnosed?
Diagnosis is usually made by the clinical appearance and by the exclusion of other similar skin conditions such as psoriasis (circumscribed red scaly plaques), pityriasis rosea (herald patch, fir-tree distribution, not affecting scalp or ears) or pityriasis versicolor (less flaky, tends to involve central trunk).
Skin swabs for bacterialculture may be taken if there are oozing areas, as these are often related to Staphylococcus aureus. Skin scrapings for mycology may show yeast forms, but may also be negative, as the hypersensitivity reaction can eliminate them.
How is pityriasiform seborrhoeide treated?
Pityriasiform seborrhoeide can be treated topically using a combination of: