
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction Demographics Causes Clinical features Complications Diagnosis Differential diagnoses Treatment Outcome
Primary cutaneous CD30+ lymphoproliferative disorders (LPD) are indolent-behaving extranodal T-cell neoplasms localised to the skin and characterised by CD30 expression on atypical lymphocytes. Lymphoproliferative disorders account for about 10% of cutaneous lymphomas and 30% of cutaneous T-cell lymphomas (CTCL). CD30+ lymphoproliferative disorders are the second most common form of CTCL after mycosis fungoides.
Primary cutaneous CD30+ lymphoproliferative disorders are classified as:


Primary cutaneous CD30+ lymphoproliferative disorders are rare. They affect both sexes, all races, and all ages. However, there are some differences in the epidemiology of the various types:
The aetiopathogenesis of primary cutaneous CD30+ lymphoproliferative disorders remains elusive. CD30 signalling is known to affect growth and survival of lymphoid cells. Some studies suggest restriction of the normal T-cell repertoire in the peripheral blood. Other hypotheses implicate reactive phenomena inducing CD30+ overexpression.
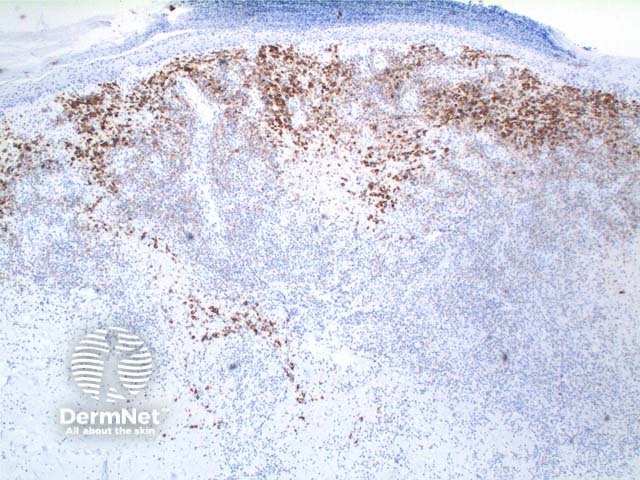
Primary cutaneous CD30+ lymphoproliferative disorders require careful clinicopathological correlation to make the diagnosis. History, examination, and skin biopsy histopathology/immunohistochemistry must be compatible. Histopathology alone is not diagnostic as similar changes can be seen in other skin disorders.
There are currently no treatments that change the natural history or cure LyP. Treatment is not always required if eruptions are infrequent, produce few lesions, and do not scar. Treatment may be considered to reduce the frequency and severity of crops or accelerate healing for frequent, extensive cropping or where there is an impact on quality of life, but needs to be weighed up against side effects.
Anti-CD30 medications such as brentuximab vedotin (anti-CD30 monoclonal antibody linked to monomethyl auristatin E) are being used increasingly in the treatment of primary cutaneous CD30+ lymphoproliferative disorders.
Primary cutaneous CD30+ lymphoproliferative disorders look malignant on histopathology but most follow an indolent clinical course. Five-year survival is estimated to be 100% for lymphomatoid papulosis and 95% for primary cutaneous anaplastic large-cell lymphoma. However, five-year survival of generalised pcALCL may be as low as 50%.
Long-term surveillance and follow-up is recommended as LyP can be associated with other cutaneous and systemic lymphomas in up to 20% of cases, and pcALCL can recur or spread beyond the skin.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more