
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Causes
Demographics
Signs and symptoms
Diagnosis
Treatment
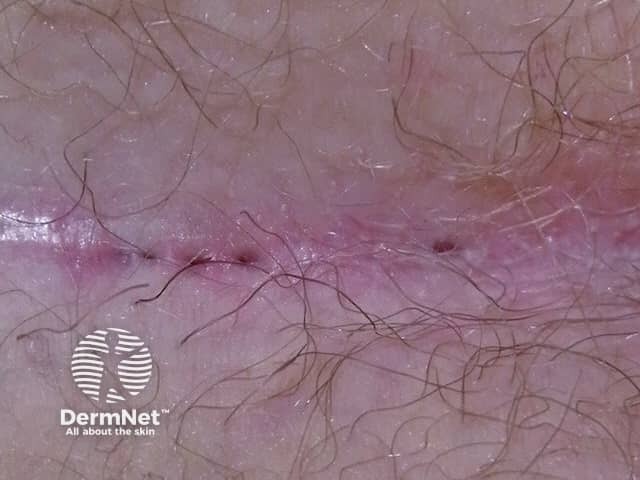
Pilonidal disease is a chronic skin problem found most often in the sacrococcygeal region. This is the cleft between the buttocks just below the base of the spine. It is characterised by one or more sinus tracts; these are cavities with a narrow opening on the skin surface (pilonidal sinus). In most cases, the cavity is filled with nests of hair – hence the name pilonidal ("pilus" meaning hair and "nidal" meaning nest). A non-inflamed lump is known as a pilonidal cyst. If the sinus becomes infected a pilonidal abscess may form.

The exact reason why pilonidal disease occurs is still unclear. Possible causes include:
Pilonidal disease affects both men and women usually between the ages of 20–40 years. It is 2–3 times more common in men than women. Other factors that increase the risk of pilonidal disease include:
Signs and symptoms can vary from a small painless pit or dimple at the base of the spine to a large painful abscess. Most patients have progressive tenderness, particularly after prolonged periods of sitting, such as during a long drive. Signs and symptoms include:
The clinical features of pilonidal sinus is usually straightforward. If necessary, skin biopsy can be undertaken. The histopathological features of pilonidal sinus characteristically show foreign body reaction.
A pilonidal cyst that isn't causing any problems doesn't require any treatment. The patient should be advised to keep the area clean and free of hair by shaving or using a hair removal agent every 2–3 weeks. The cyst may resolve itself. Persistent and inflamed cysts (acute pilonidal abscess) are incised (cut into) and drained out to reduce inflammation and pain. Occasionally the abscess cavity may be cut out completely to remove hair nests and skin debris; this reduces the rate of recurrence to about 15%.
Persistent, complex or recurrent pilonidal sinus disease must be treated surgically. Procedures vary from taking the roof off the sinuses to wide and deep excision (ie all affected areas are completely cut out). In all cases, the cavity is scrubbed and scraped out to remove hair and abnormally healing granulation tissue. Several techniques are available for wound healing and closure; these include
Laser hair depilation may also be a safe and effective postoperative adjunct treatment for sacrococcygeal pilonidal sinus disease.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more