Pilonidal sinus is a common condition typically affecting the region of the base of the spine or the interglutealcleft. Other anatomic sites have been rarely reported. It is regarded by many authors within the “follicularocclusion tetrad” as the primary process appears to be follicular occlusion.
Histology of pilonidal sinus
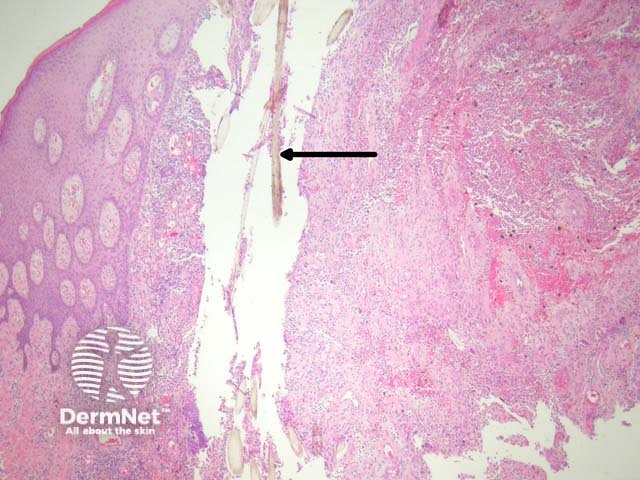
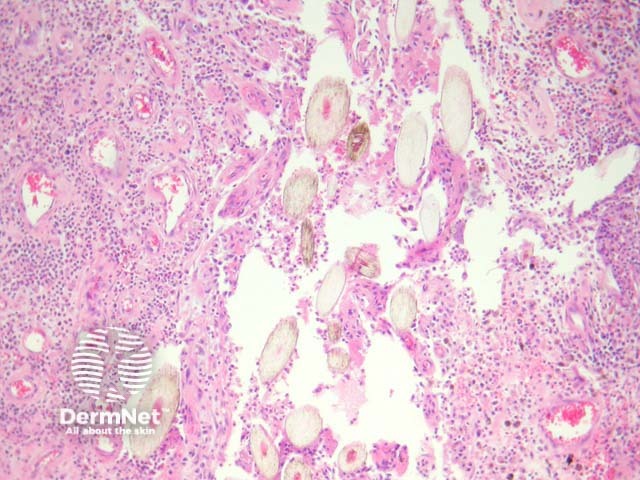
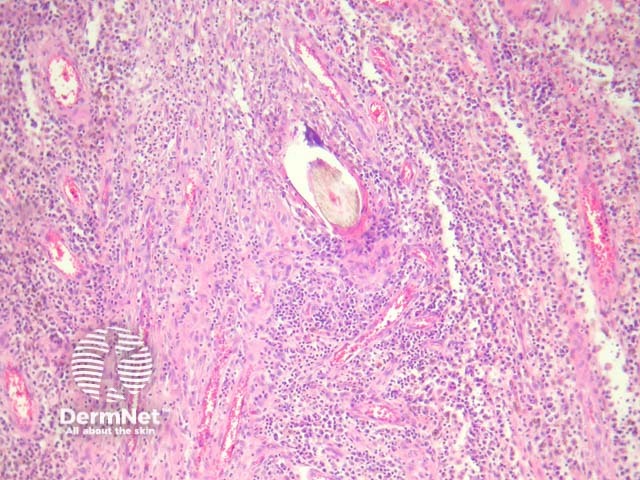
Sections show a dense inflammatory reaction usually occupying the entire dermis with erosion and ulceration of the overlying epidermis (figure 1). Free hair shafts are often seen coursing through the inflammatory focus (figure 2, arrow). Often, the free hair shafts are seen in clusters (figure 3). Dye used to outline the sinus tract for the surgeon may sometimes be seen. Surrounding the free hair shafts is a polymorphousinfiltrate which may be rich in plasma cells and lymphocytes (figure 4). Foreign body-type giant cells and neutrophilicabscesses are also commonly observed.
Figure 1
Figure 2
Figure 3
Figure 4
Special studies for Pilonidal sinus
None are generally needed.
Differential diagnosis of pilonidal sinus pathology
Follicular occlusion tetrad – Hidradenitis suppurativa (acne inversa), acne conglobata (severe nodulocystic acne), dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens) will show a similar histopathology. Correlation with the clinical findings is helpful.
Squamous cell carcinoma – Squamous cell carcinoma has been reported to occur within pilonidal sinuses. Though rare, careful examination of the squamous epithelium, particularly in cases with a marked epithelial reaction pattern is prudent.
References
Weedon’s Skin Pathology (Third edition, 2010). David Weedon
Pathology of the Skin (Fourth edition, 2012). McKee PH, J. Calonje JE, Granter SR