
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Causes
Clinical features
Complications
Diagnosis
Assessment of severity
Treatment
Outcome
Pemphigus vulgaris is a rare autoimmune disease that is characterised by painful blisters and erosions on the skin and mucous membranes, most commonly inside the mouth. Pemphigus vulgaris accounts for 70% of all pemphigus cases worldwide although it is extremely rare in New Zealand (about one case per million of the population).
The other main subtypes of pemphigus are:
Pemphigus foliaceus and allied disorders
Pemphigus vulgaris and allied disorders


See more pemphigus vulgaris images
Pemphigus vulgaris affects people of all races, age, and sex. It most commonly appears between the ages of 30 and 60 years and is more common in Jews and Indians than in other races, presumably for genetic reasons.
Drug-induced pemphigus is also recognised and is most often caused by penicillamine, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and cephalosporins.
Pemphigus is sometimes triggered by cancers particularly lymphomas and Castelman disease (paraneoplastic pemphigus), infection, or trauma.
Pemphigus vulgaris is an autoimmune blistering disease.
The keratinocytes are cemented together at unique sticky spots called desmosomes. In pemphigus vulgaris, immunoglobulin type G (IgG) autoantibodies bind to a protein called desmoglein 3 (DSG3), which is found in desmosomes in the keratinocytes near the bottom of the epidermis. The result is the keratinocytes separate from each other, and are replaced by fluid (the blister). About 50% of patients with pemphigus vulgaris also have anti-DSG1 antibodies. Large epidemiological studies have suggested a rare link between herpes virus infection and pemphigus.
Most patients with pemphigus vulgaris first present with lesions on the mucous membranes such as the mouth and genitals. Blisters usually develop on the skin after a few weeks or months, although in some cases, mucosal lesions may be the only manifestation of the disease.
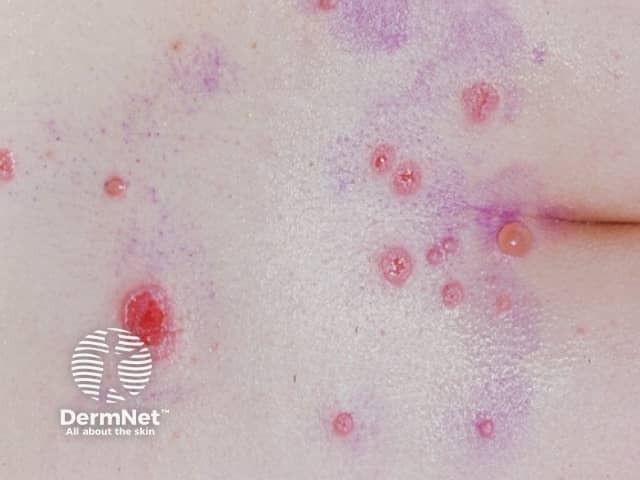
Skin lesions appear as thin-walled flaccid blisters filled with clear fluid that easily rupture causing itchy and painful erosions. They most often arise on the upper chest, back, scalp, and face. Erosions in the skin folds may develop into vegetative lesions which are granular and crusted (pemphigus vegetans). The skin around the nails may be painful, red, and swollen.



In comparison to white skin, darker skin tones may differ in their presentation which can cause diagnostic delay. Diagnostic features in darker skin tones may include flaccid blister which lack erythema and hyperpigmented plaques with superficial erosion and haemorrhagic crusting. At later and more advanced stages, plaques with a pink base and surrounding hyperpigmentation are present.
The inside of the mouth is commonly involved in pemphigus vulgaris. Involvement of the pharynx and larynx cause pain on swallowing and a hoarse voice. Nasal involvement causes congestion and bleeding. The conjunctiva, oesophagus, labia, vagina, cervix, penis, urethra and anus may also be affected.
Features of oral mucosal pemphigus include:



See more pemphigus vulgaris images
Pemphigus vulgaris can cause very extensive, life-threatening erosions, especially if the diagnosis is delayed. Other potentially severe complications may include:
Diagnosis of pemphigus vulgaris generally requires a biopsy of a blister. Diagnosis of pemphigus vulgaris generally requires a biopsy from the skin adjacent to a lesion. Histology typically shows rounded-up and separated keratinocytes (acantholytic cells) just above the basal layer of the epidermis. Suprabasal clefting may be reported. See pathology of pemphigus vulgaris.
Pemphigus is confirmed by direct immunofluorescence staining of perilesional skin biopsy sections to reveal immunoglobulin (Ig)G antibodies or complement on the cell surfaces of keratinocytes.
In most cases, circulating antibodies can be detected by a blood test (indirect immunofluorescence test). The level of antibodies fluctuates and may reflect the effectiveness of treatment. Specific anti-dsg1 and anti-dsg3 antibody titres can also be measured in blood or saliva by enzyme-linked immunosorbent assays (ELISAs).
Pemphigus vulgaris may co-exist with or be confused with pemphigus foliaceus, cicatricial pemphigoid and lichen planus.
The severity of pemphigus can be scored using various scoring systems.
The primary aim of treatment of pemphigus vulgaris is to decrease blister formation, prevent infections and promote healing of blisters and erosions [4.5]. Systemic corticosteroids >are the mainstay of medical treatment for controlling the disease, usually in the form of moderate to high doses of oral prednisone or prednisolone, or as pulsed intravenous methylprednisolone. Since their use, many deaths from pemphigus vulgaris have been prevented (the mortality rate dropped from 99% to 5–15%). Corticosteroids are not a cure for the disease but improve the patient's quality of life by reducing disease activity. The doses of corticosteroids needed to control pemphigus vulgaris and the length of time on treatment may result in serious side effects and risks.
Other immunosuppressive drugs (mostly off-label) used to reduce the dose of steroids and may be required by patients with pemphigus vulgaris for years. These are most often:
Other medications that are sometimes used in pemphigus (often in combination) include:
At optimal therapy, patients may continue to experience mild disease activity.
Other considerations include vaccination (live vaccines are contraindicated), bone prophylaxis, baseline ophthalmological assessment, and psychological support if needed.
Topical therapy for cutaneous pemphigus vulgaris may include topical steroids and emollients.
Treatment of mucosal pemphigus vulgaris may include various formulations of a topical steroid, intralesional steroid, topical tacrolimus, or topical ciclosporin.
Appropriate wound care is particularly important, as this should promote healing of blisters and erosions.
Patients should minimise activities that may traumatise the skin and mucous membranes during active phases of the disease. These include activities such as contact sports and eating or drinking food that may irritate or damage the inside of the mouth (spicy, acidic, hard and crunchy foods).
Oral hygiene and proper dental care are essential.
There is future hope that future treatment for pemphigus will be more specific with fewer side effects. The CD20 antagonist ofatumumab has been reported to be effective. Investigators have engineered specific chimeric autoantibody receptor T-cells to eliminate desmoglein-3-specific B cells in mice. The use of anti-neonatal Fc receptor is under investigation in combination with rituximab.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more