Pemphigus vulgaris is a chronicvesiculobullous skin disorder characterised by autoantibodies against desmoglein 3, which is a component of the desmosome (an intracellularadhesionmolecule). Disruption of keratinocyte adhesion leads to superficial blistering and erosion affecting the skin and/or mucous membranes.
Histology of pemphigus vulgaris
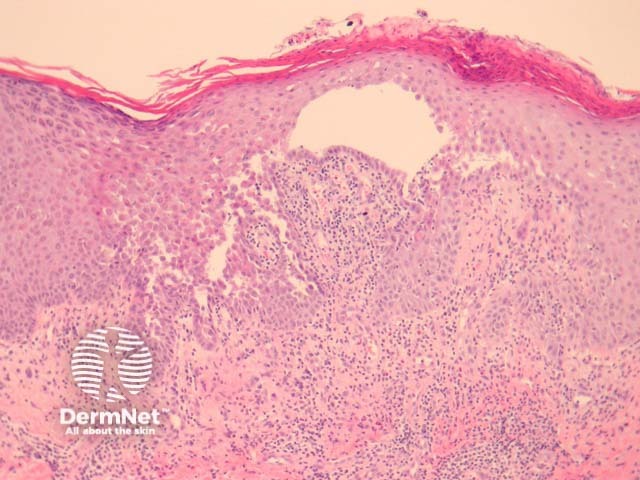
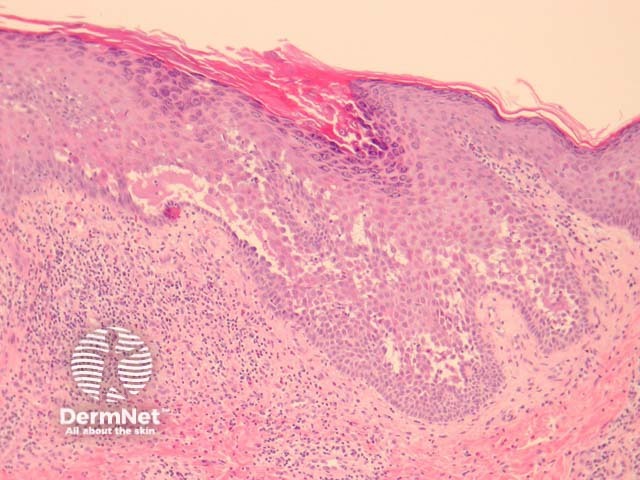
Early lesions of pemphigus vulgaris show suprabasalepidermalacantholysis, clefting and blister formation. The blister cavity may contain inflammatory cells including eosinophils and rounded acantholytic cells with intensely eosinophiliccytoplasm and a perinuclear halo. The floor of the blister may be lined with intact keratinocytes, the “tombstone pattern” (figures 1, 2). Acantholysis can also affect adnexae.Dermal changes include perivascular inflammatory infiltrate particularly with eosinophils.
Figure 1
Figure 2
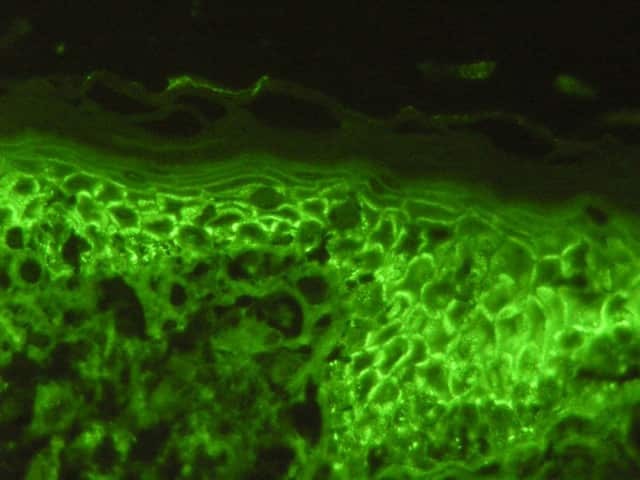
Figure 3
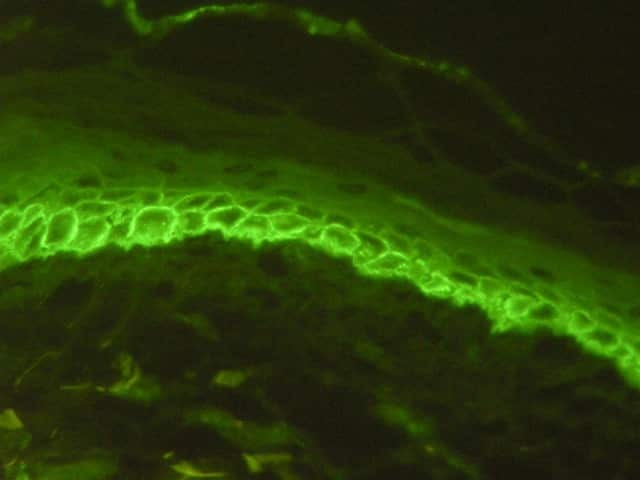
Figure 4
Special studies of pemphigus vulgaris
Direct immunofluorescence may be positive in perilesional skin with intercellular deposits of IgG and/or C3 in the epidermis (figures 3, 4). Antigendeposition can be seen in hairfollicles (follicular outer root sheath and germinal matrix), meaning direct immunofluorescence may be positive when performed on plucked hair follicles.
Differential diagnosis of pemphigus vulgaris
Darier disease: Suprabasal clefting with dyskeratosis in the form of corps ronds and grains. Immunofluorescence is negative.
Hailey-Hailey disease: Disruption of epitheliumadjacent to bullae (intact in pemphigus vulgaris) with sparing of adnexal structures. Immunofluorescence is negative.
Pemphigus foliaceus: Acantholysis more superficial within the granular layer. Lacks mucous membrane involvement.
Grover disease: There is a pemphigus-like form of this disease. Negative immunofluorescence and lack of adnexal involvement are helpful features.