
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction Demographics Causes Clinical features Complications Diagnosis Treatment Outcome
Crusted scabies is a highly contagious hyperinfestation with Sarcoptes scabiei var hominis presenting in immune compromised patients.
Crusted scabies was formerly known as Norwegian scabies.
Scabies is passed on from another individual infested by scabies mites. Crusted scabies may arise in people who fail to mount a normal immune response to the mites.
Crusted scabies is prevalent in remote Aboriginal communities in Northern Australia.
Risk factors for crusted scabies include:
It may also result from misdiagnosis as psoriasis or seborrhoeic dermatitis and treatment of these disorders.
It is estimated that individuals with crusted scabies have up to 4,000 mites per gram of skin. Patients are often infected with over 1 million mites. Compare this to the majority of patients with scabies, who are infected with around 10–20 mites.
The exact reason why crusted scabies arises is unknown. It is associated with elevated eosinophils, IgE, and IgG. The dermis is infiltrated with lymphocytes and eosinophils. There is an increased ratio of CD8+ lymphocytes compared to normal.
Crusted scabies begins as poorly defined red patches that then develop into thick scaly plaques between the fingers, under the nails, or diffusely over palms and soles. Other common areas include elbows and knees. Mites can also collect in nail beds, causing the nail plates to split.





Itching in crusted scabies may be minimal or absent. This may be due to the immune compromised nature of the individual. The following can contribute to the reduction in scratching:
Complications of crusted scabies include:
Scabies is readily diagnosed clinically and confirmed by identification of mites or eggs on dermoscopic or microscopic examination of burrows. Reflectance confocal microscopy has also been used to examine for burrows, mites, eggs, and mite faeces.
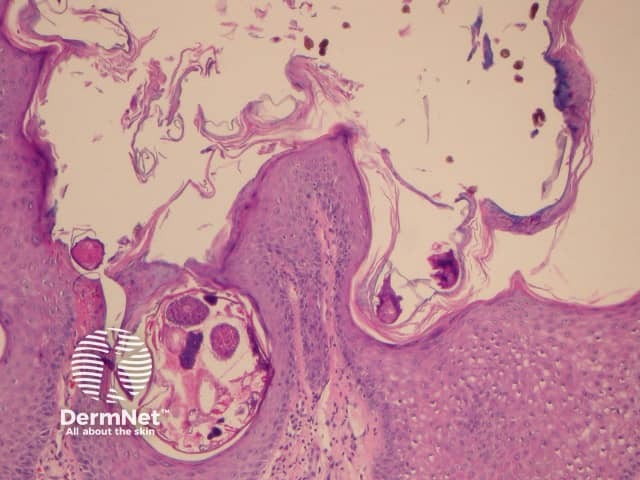
Skin biopsy is rarely necessary, and will show characteristic crusted scabies pathology.
A dermatologist or infectious disease physician should be involved in the care of the patient and contacts. Treatment of crusted scabies should be done in an inpatient or residential setting, with the patient in a private room. Healthcare staff should take contact precautions and wear full personal protective equipment, including shoe and hair covers.
Treatment requires oral ivermectin and topical insecticides. The following grading system devised at the Royal Darwin Hospital may be used to determine the protocol.
A: Distribution
B. Crusting/shedding
C. Past episodes
D. Skin condition
Grade 1: total score 4–6
Grade 2: total score 7–9
Grade 3: total score 10–12
The dose of ivermectin is 200 μg/kg for adults and children over 14 kg, rounded up to nearest 3 mg, and taken after a fatty meal to aid absorption.
A topical scabicide is applied every second day for the first week, and then twice a week until cured.
Keratolytic creams are used on scaly plaques on alternate days to scabicide. First, soften crusts in warm water. Then apply either:
The treating dermatologist or infectious disease physician should carefully re-examine the patient to decide when to stop treatment.
A combination regimen for the treatment of crusted scabies devised by the US Centers for Disease Control (CDC) recommends:
AND
Family members should also be screened for crusted scabies, and treated accordingly. Regardless of examination findings, all family members should be treated with a topical scabicide, and should repeat treatment in one week.
Mites can survive for up to 72 hours away from a human host. Living areas should be thoroughly cleaned, as crusted plaques will commonly be shed. Linen and mattresses should also be cleaned.
Treatment will cure crusted scabies. However, patients with crusted scabies are at risk of reinfestation due to their immune status and living conditions. Education and regular follow-up are essential.
Mortality is significantly higher in older patients with crusted scabies in comparison with patients that have regular scabies. Disease-related mortality is attributed to sepsis.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more