Author: Dr Kate Quirke, Senior House Officer, Rotorua Hospital, New Zealand. Copy edited by Gus Mitchell. March 2022. Previous author: Hon A/Prof Amanda Oakley, Dermatologist, Waikato Hospital, New Zealand.
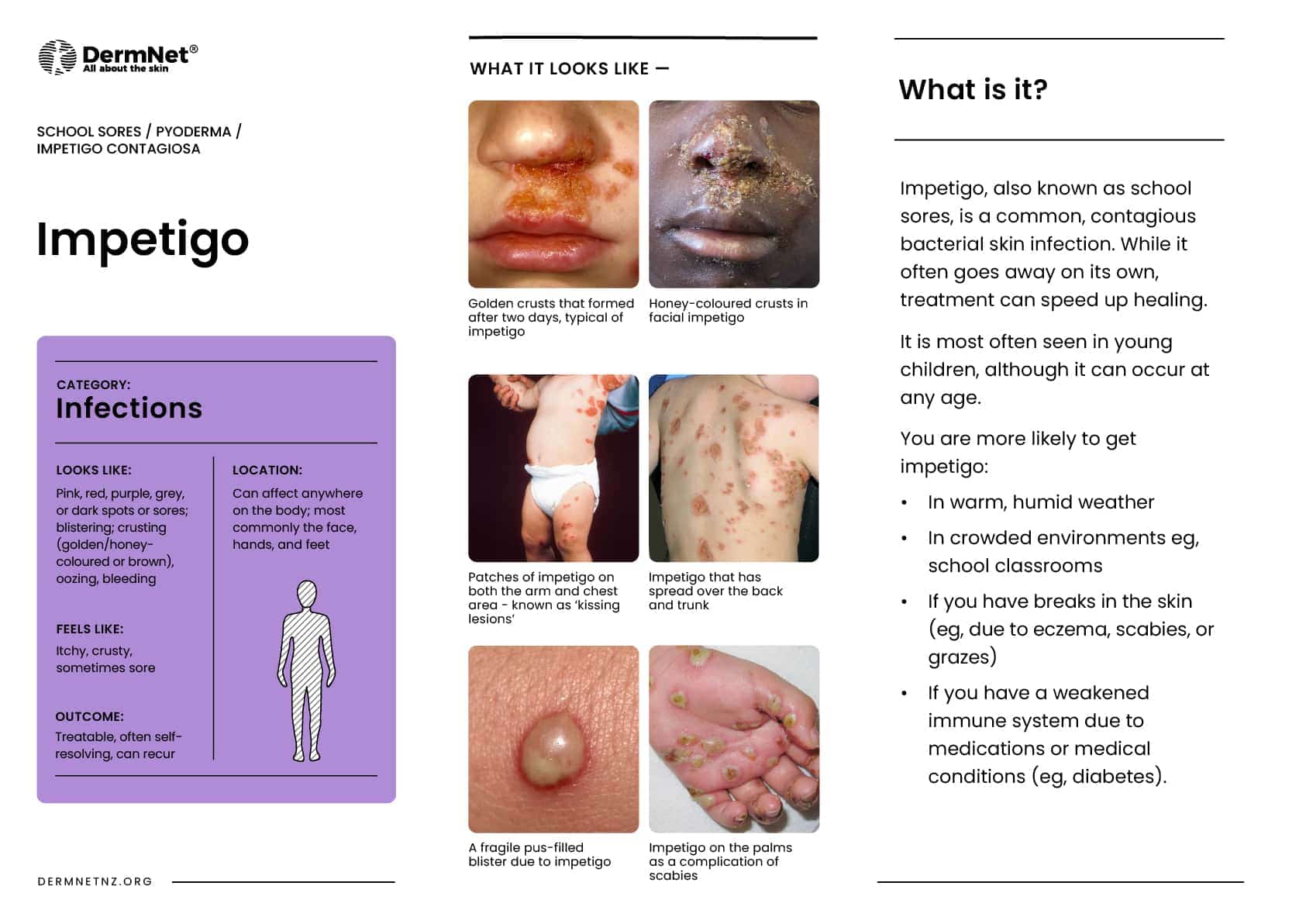
Impetigo is a common, superficial, highly contagious bacterial skin infection characterised by pustules and honey-coloured crustederosions.
It affects the superficial layers of the epidermis and is typically caused by Staphylococcus aureus and Streptococcus pyogenes (Group A beta – haemolytic streptococci (GABHS)). It can be classified into non-bullous (also known as ‘school sores’) and bullous impetigo. Ecthyma is a deep form of impetigo causing deeper erosions of the skin into the dermis.
Secondary infection of wounds or other skin lesions with the same pathogens is called ‘impetiginisation’.
Honey-coloured crusts on the chin in impetigo
'Kissing lesions' on both sides of the axilla in impetigo
Perioral honey-coloured crusts in impetigo
Widespread bullous impetigo over the back
An intact blister and erosions in bullous impetigo
Caused by either Staphylococcus aureus, Streptococcus pyogenes, or both bacteria conjointly.
Intact skin is usually resistant to colonisation from bacteria. Disruption in skin integrity allows for invasion of bacteria via the interrupted surface.
Bullous impetigo
Due to Staphylococcus aureus which produces exfoliativetoxins (exfoliatins A and B).
Exfoliative toxins target intracellularadhesionmolecules (desmoglein – 1) present in the epidermalgranular layer.
Results in dissociation of epidermal cells which causes blister formation.
Can occur on areas of intact skin.
What are the clinical features of impetigo?
Non-bullous impetigo
Most commonly found on the face or extremities but skin on any part of the body can be involved.
Begins with a single erythematousmacule which evolves into a pustule or vesicle.
Pustule or vesicle ruptures releasing serous contents which dries leaving a typical honey-coloured crust.
Minimal or no surrounding erythema.
Can spread rapidly with satellite lesions due to autoinoculation.
“Kissing lesions” arise where two skin surfaces are in contact.
Patients are typically otherwise well; they may experience some itching and regional lymphadenopathy.
Bullous impetigo
Usually found on the face, trunk, extremities, buttocks, and perineal regions.
Can spread distally due to autoinoculation.
Present as quickly appearing superficial, small or large thin roofed bullae which tend to spontaneously rupture and ooze yellow fluid leaving a scaley rim (collarette).
More likely to have systemic symptoms of malaise, fever, and lymphadenopathy.
Crusted weepy lesions in facial impetigo
Impetigo on the leg
Facial impetigo
How do clinical features vary in differing types of skin?
The initial erythematous macule in non-bullous impetigo may be more difficult to see on darker skin tones.
What are the complications of impetigo?
Wider spread infection: cellulitis, lymphangitis, and bacteraemia.
Post-streptococcal glomerulonephritis: a rare, acuterenal condition following infection with Streptococcus pyogenes (group A streptococcus). This is due to a type III hypersensitivity reaction and presents 2–6 weeks post-skin infection.
Regular gentle cleansing; removal of honey-coloured crusts.
Practice good hand hygiene and keep fingernails cut short.
Cover the affected areas with watertight dressing to prevent spread.
Specific measures
Topical antibiotics
For localised non-bullous impetigo, application of antiseptic 2–3 times per day for 5–7 days is recommended (e.g. hydrogen peroxide 1% cream or povidone — iodine 10% ointment).
Topical antibiotics such as fusidic acid or mupirocin are effective in treating non-bullous impetigo, however, their use may not be recommended in some countries due to bacterial resistance.
Topical antibiotics can be considered when antiseptic treatment has not worked or is not appropriate (e.g. impetigo around the eyes).
Fusidic acid is first-line.
Mupirocin use is often reserved for possible MRSA infection.
Oral antibiotics
Recommended in bullous impetigo, widespread non-bullous impetigo (>3 lesions), when topical treatment fails, a person is at high risk of complications, or when a person is systemically unwell.
Oral flucloxacillin is often the first line antibiotic of choice.
Alternatives may include trimethoprim + sulfamethoxazole or erythromycin (eg, if penicillin allergic or for MRSA infection).
Preventative measures
Avoid touching affected areas.
Practice good hand hygiene; wash hands before and after applying creams.
Use a clean cloth each time to wash and dry affected areas.
Do not share towels or face cloths.
Clothing and bedding should be changed daily; wash using hot temperatures.
Avoid close contact with others — school/nursery children should stay home until lesions have crusted over, or they have received at least 24 hours of treatment.
What is the outcome for impetigo?
Impetigo is usually self-limiting without serious complications. Without treatment, impetigo usually heals in 2–3 weeks; with treatment lesions resolve within 10 days.
Postinflammatoryhypopigmentation or hyperpigmentation may occur but scarring is uncommon.
Bibliography
Bowen AC, Mahé A, Hay RJ, Andrews RM, Steer AC, Tong SYC, Carapetis JR. The Global Epidemiology of Impetigo: A Systematic Review of the Population Prevalence of Impetigo and Pyoderma. PLoS One. 2015;10(8):e0136789. Journal
Cole C, Gazewood J: Diagnosis and Treatment of Impetigo. Am Fam Physician. 2007;75(6):859–64. Journal
Hartman-Adams H, Banvard C, Juckett G. Impetigo: diagnosis and treatment. Am Fam Physician. 2014;90(4):229–35. Journal
Hoffmann TC, Peiris R, Glasziou P, Cleo G, Mar CD. Natural history of non-bullous impetigo: a systematic review of time to resolution or improvement without antibiotic treatment. Br J Gen Pract. 2021;71(704):e237–42. Journal
Kato F, Kadomoto N, Iwamoto Y, Bunai K, Komatsuzawa H, Sugai M. Regulatory mechanism for exfoliative toxin production in Staphylococcus aureus. Infect Immun. 2011;79:1660–70. Journal
Williamson D, Ritchie S, Best E, Upton A, Leversha A, Smith A, Thomas M. A bug in the ointment: topical antimicrobial usage and resistance in New Zealand. N Z Med J. 2015;128:103–9. Journal