
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction How it works Uses Features observable with OCT Features not observable with OCT Skin conditions assessed
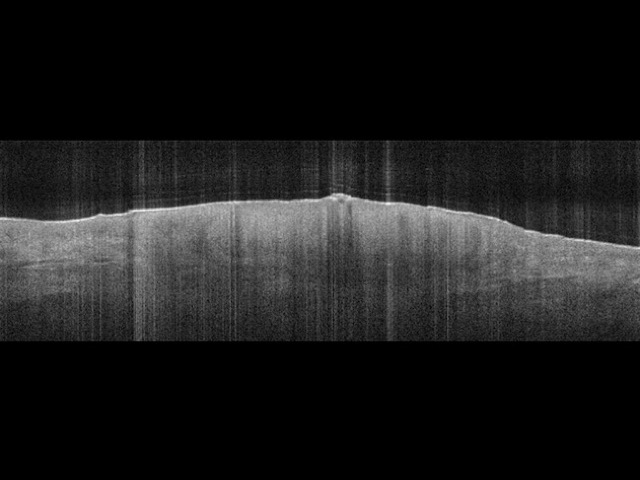
Optical coherence tomography (OCT) is a non-invasive optical imaging technique that uses low-power infrared laser light to image up to 2 mm beneath the skin surface. The clinician can obtain real-time images of the architecture of the skin without pretreatment or gels.
OCT has been shown to be a useful diagnostic tool in diagnosing early stage skin cancer [1]. What lies beneath the skin surface can be seen in vivo, without the need for skin biopsy [2]. Studies have compared OCT findings with histopathology, establishing the OCT characteristics of actinic keratoses, in-situ squamous cell carcinoma (SCC), and basal cell carcinoma (BCC) [1].
Benefits of OCT imaging include differentiating abnormal from normal tissue in vivo, and monitoring the site after treatment of nonmelanoma skin cancers [3].



Images courtesy of Michelson Diagnostics and *Dr Orit Markowitz
OCT imaging is similar to ultrasound, in that it measures echo delays and creates A-scan images via interferomic analysis. In OCT, a light beam is directed at the area of interest in the skin, rather than sound or radio frequency.
Most light is not reflected from skin structures, but scatters off at large angles. In conventional imaging, this diffusely scattered light contributes background that obscures an image. In OCT, interferometry is used to record the optical path length of received photons, allowing rejection of background photons that scatter multiple times. Thus OCT can build up clear 3D images of thick samples by only collecting light that is directly reflected from surfaces of interest.
The mechanism of producing an OCT image is described here:
The main uses of OCT are to evaluate and monitor:
OCT has been particularly useful in delineating excision margins prior to Mohs surgery for BCC. In combination with clinical examination and dermatoscopy:
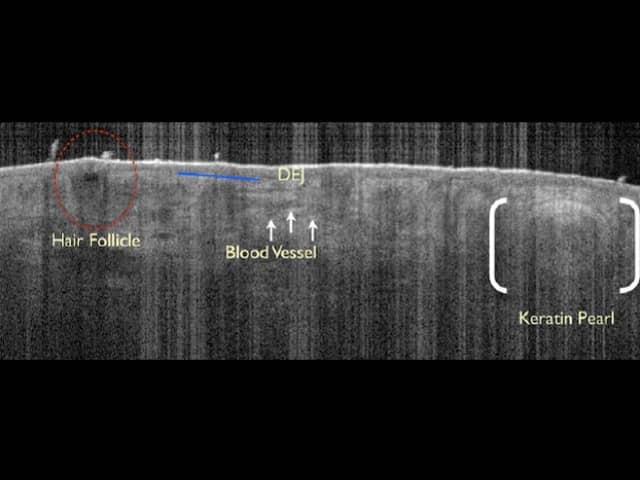
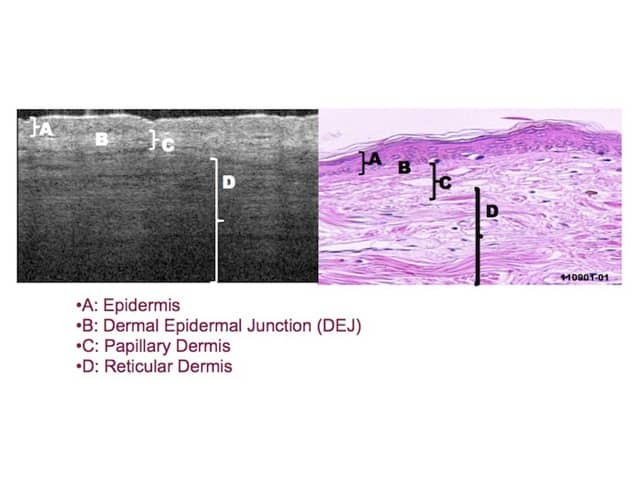
Imaging with OCT can clearly differentiate the epidermis from the upper dermis, so that selected skin areas can be accurately measured. OCT reveals:
Images courtesy Dr Orit Markowitz1, Michelson Diagnostics2
The vertical field of view of OCT equates to a width of up to 10mm and a depth of 1 to 2mm.
OCT provides architectural information, but it does not provide single-cell resolution within the skin.
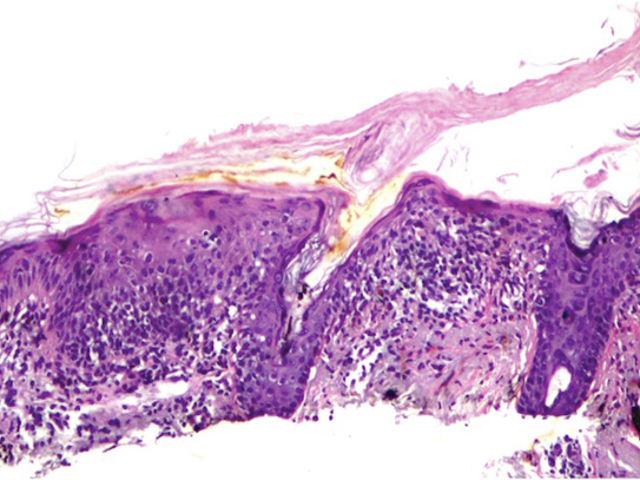
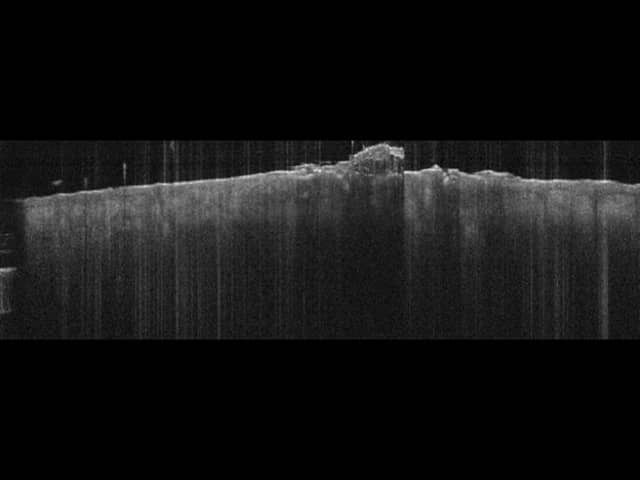
Pigmented lesions show regular scattering patterns on OCT. OCT is not suitable for diagnosis of pigmented lesions, as specific criteria to distinguish benign from malignant lesions are currently lacking. However, OCT has been used to measure tumour thickness in thin melanomas.
Images courtesy of Dr Orit Markowitz
A 2010 study demonstrated that OCT measurements of epidermal thickness in psoriatic plaques correlated with several parameters of disease severity [5]. This implies that OCT imaging may be useful to assess psoriasis during treatment.
OCT imaging is a reliable non-invasive tool for identifying fungal elements in onychomycosis [6]. Preliminary studies have shown OCT can assess the severity of psoriatic nail disease in plaque psoriasis and psoriatic arthritis.
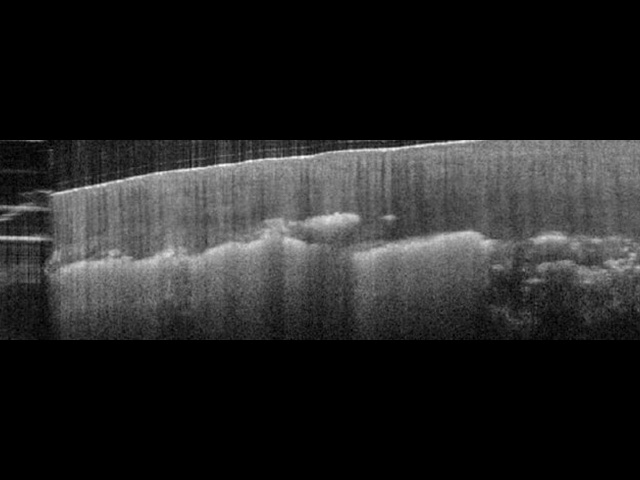
Image courtesy of Dr Orit Markowitz
In-vivo OCT imaging of the skin may prove useful in the assessment of systemic sclerosis [7]. OCT can be used to identify the DEJ, measure the degree of fibrosis and assess the blood vessels.
Nonmelanoma skin cancers such as actinic keratoses and BCCs are the primary indications for OCT. It can be used for diagnosis, to determine the depth of tumour infiltration and the width of the tumour, and to monitor the response to topical treatments. As OCT imaging is non-invasive, patients may be spared from unnecessary repetitive biopsies.
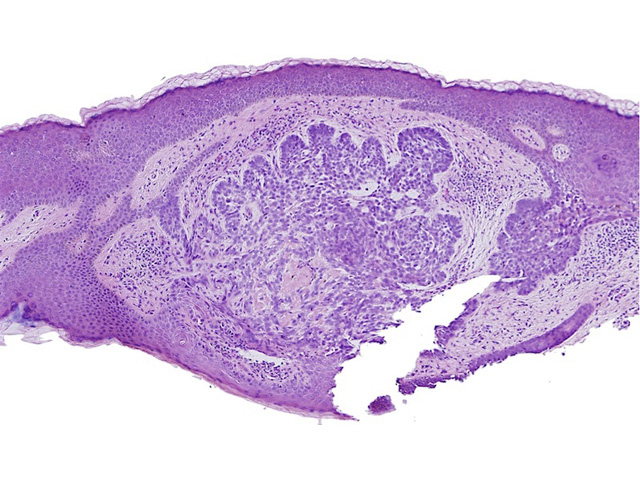
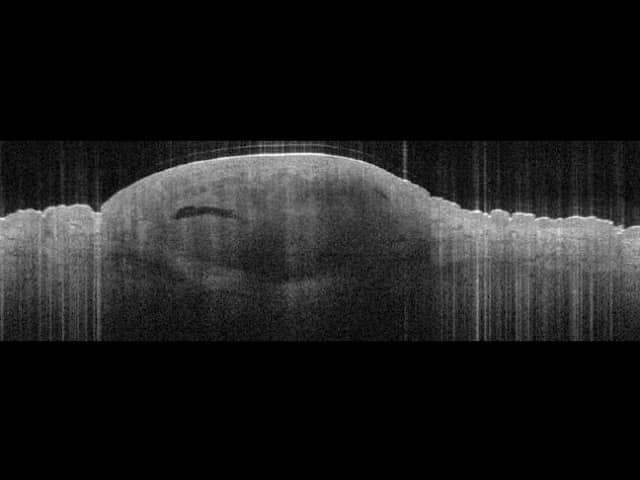
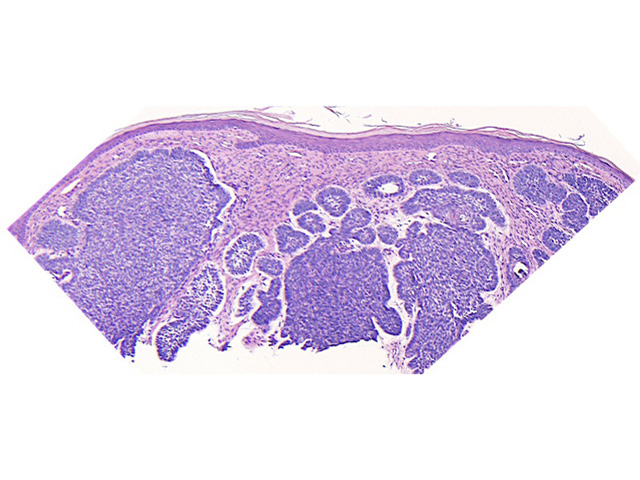
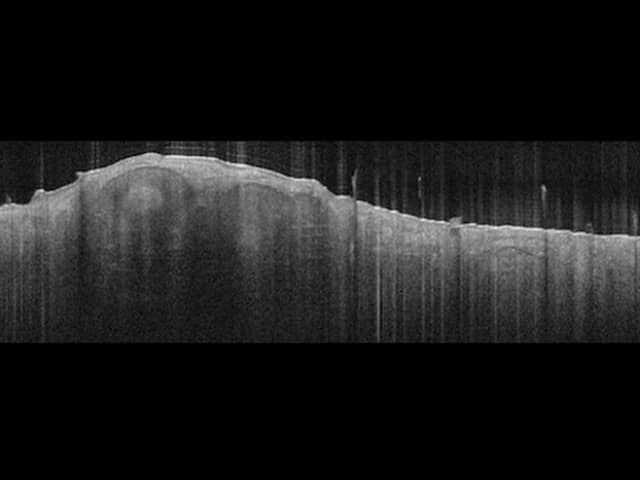
Images courtesy of Dr Orit Markowitz. In the right hand example, the dark halo encompassing the BCC tumour on OCT (bottom) is a characteristic finding for BCC nests. This feature includes both the mucinous cleft and the peripheral palisading evident on histology sections (top).
The potential applications of non-invasive imaging with OCT span a wide range of medical, surgical, and cosmetic aspects of dermatology. For example, OCT has been demonstrated to provide useful information in measuring and monitoring:
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more