Authors: Vanessa Ngan, Staff Writer, 2005; Updated: Dr Aswan Tai, Peter MacCallum Cancer Centre, Melbourne, Australia; Dr Sarah Smithson, Dermatologist, Skin Health Institute, Melbourne, Australia. Copy edited by Gus Mitchell. April 2022
Kyrle disease was first described in 1916 by Austrian dermatologist and pathologist Josef Kyrle as “hyperkeratosis follicularis et parafollicularis in cutem penetrams” in a diabetic female patient with generalisedhyperkeratoticpapules.
There is longstanding controversy surrounding the classification of Kyrle disease, with some clinicians believing it to be a distinct clinical entity and others considering it as within the reactive perforating collagenosis spectrum.
Who gets Kyrle disease?
Can affect both males and females throughout life.
Onset is usually in adulthood around 30 years of age.
No clear racial predilection.
Strong association with diabetes mellitus, chronicrenal disease, chronic liver diseases, and congestive heart failure.
What causes Kyrle disease?
The pathogenesis of Kyrle disease (KD) is unclear.
The keratinization process in KD is altered, occurring at the basal layer in the epidermis.
Abnormal keratin elicits a hostinflammatory response higher in the epidermis.
Keratin and other materials are eliminated through the epidermis.
The presence of altered or abnormal connective tissue may be a predisposing factor in KD.
Immune dysregulation in chronic renal failure may contribute to the development of KD through increased expression of interleukin (IL)-31, a predominately T-cell-derived cytokine strongly correlated with itch provocation.
What are the clinical features of Kyrle disease?
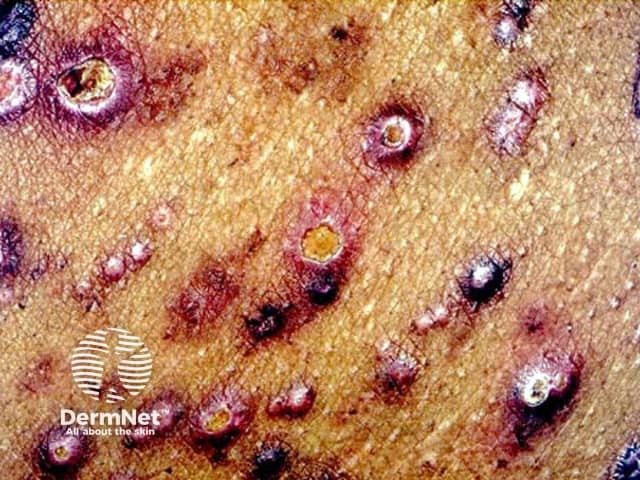
Kyrle disease is a papulonodular mucocutaneous disorder.
Red-brown papules and nodules with silvery scales, commonly with central keratin (horny) plug.
Lesions vary in shape and size and can grow up to 1.5cm in diameter.
Lesions are not normally painful or tender but can be intensely itchy.
Mostly located on the extensor surface of lower limbs but can also develop on the arms as well as head and neck region. Rarely on the palms, soles, and mucous membrane.
Kyrle disease can usually be diagnosed on its distinct clinical features, associated conditions, and confirmed on skin biopsy with histopathology showing incomplete keratinisation and a hyperkeratotic, parakeratotic plug.
What is the differential diagnosis for Kyrle disease?
The main aim of treatment is to control itch and avoid superficial trauma. Rapid improvement and resolution of lesions are often seen once any associated underlying disease is managed.
Clinical trial — immunomodulatory drugs (eg, IL-31 monoclonalantibodies such as nemolizumab).
What is the outcome for Kyrle disease?
Lesions are self-healing but often recur. Individuals can develop larger and more lesions with age.
References
Ataseven A, Ozturk P, Kucukosmanoglu I, Kurtipek GS. Kyrle's disease. BMJ Case Rep. 2014;2014:bcr2013009905. Published 2014 Jan 15. doi:10.1136/bcr-2013-009905. PubMed
Bodman M, Ehredt D Jr, Barker R, Kirkland A, Mude P. Kyrle Disease A Rare Dermatologic Condition Associated with the Diabetic Foot. J Am Podiatr Med Assoc. 2015;105(5):451-455. doi:10.7547/14-009. PubMed
Forouzandeh M, Stratman S, Yosipovitch G. The treatment of Kyrle's disease: a systematic review. J Eur Acad Dermatol Venereol. 2020;34(7):1457–63. doi:10.1111/jdv.16182. Journal
Rapini RP, Herbert AA, Drucker CR. Acquired perforating dermatosis. Evidence for combined transepidermal elimination of both collagen and elastic fibers. Arch Dermatol. 1989;125(8):1074–8. doi:10.1001/archderm.125.8.1074. Journal
Rice AS, Zedek D. Kyrle Disease. In: StatPearls. Treasure Island (FL): StatPearls Publishing; June 4, 2021. Book