
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction - lymphoma
Introduction
Classification
Demographics
Causes
Clinical features
Cutaneous manifestations
Differential diagnoses
Treatment
Outcome
Lymphomas are cancers that develop in the lymphatic system of the body. These cancers form when there is abnormal and excessive growth of B lymphocytes and T lymphocytes in the lymph nodes and other parts of the body. There are many different subtypes of lymphoma, categorised into Hodgkin lymphoma and non-Hodgkin lymphoma (NHL).
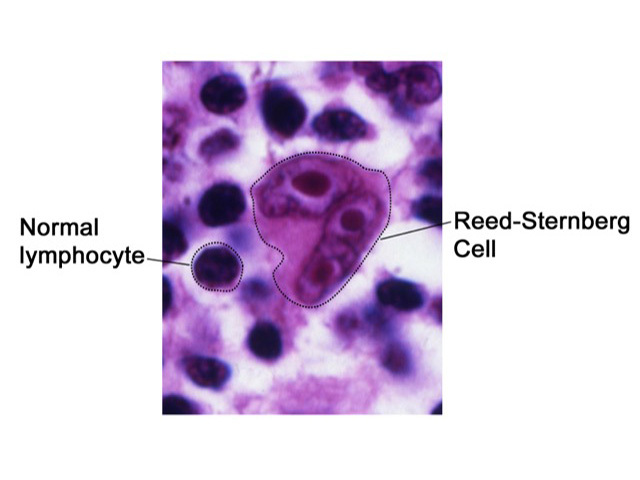
Hodgkin lymphoma is a B-cell lymphoma characterised by a tumour cell called the Reed-Sternberg cell [1]. These are large abnormal lymphocytes with multiple nuclei that are found on the histology of affected lymph nodes.
Hodgkin lymphoma typically presents with painless swelling of superficial lymph nodes or with an asymptomatic mass on a chest X-ray. Patients with Hodgkin lymphoma occasionally present with severe generalised pruritus or with skin lesions.
There are two distinct types of Hodgkin lymphoma according to the World Health Organization (WHO) Classification of Tumours of Haematopoietic and Lymphoid Tissues [2]; these being:
Classical Hodgkin lymphoma is further histologically classified into:
Hodgkin lymphoma is a relatively rare disease, accounting for approximately 0.6% of all cancers diagnosed in the developed world annually.
Hodgkin lymphoma develops in two main age groups.
Hodgkin lymphoma is caused by a change in the DNA of a B-cell lymphocyte. This mutation causes a large number of abnormal and oversized B cells to accumulate in the lymphatic system, and, over time, spread to other organs. It is not clear what causes DNA mutation.
Hodgkin lymphoma usually starts within a single lymph node and then progresses to nearby lymph nodes via the lymphatic channels before spreading to distant sites and organs [8,9]. It typically presents with painless swelling of superficial lymph nodes (in the neck, axilla, or groin) or as an asymptomatic mass seen on a chest X-ray.
Some patients present to their doctors with non-specific, or 'B', symptoms. They can have one or more of the following symptoms:
Occasionally, patients can present with symptoms and signs that reflect the involvement of organs in the disease such as:
Nonspecific cutaneous signs include:



How is Hodgkin lymphoma diagnosed?
A thorough history and physical examination is the initial step in the diagnosis of Hodgkin lymphoma, which is confirmed by the presence of Reed-Sternberg cells on the pathological examination of a lymph node biopsy [8].
Any disease presenting with enlarged lymph nodes with constitutional symptoms, such as fevers and weight loss, should be considered in the differential diagnosis of Hodgkin lymphoma [12].
The treatment for Hodgkin lymphoma may include [12]:
Chemotherapy involves either taking oral tablets or the drug is injected into a vein or muscle, depending on the type and stage of the cancer being treated.
Radiation therapy can be used to treat solitary or localised specific skin lesions. For a pregnant woman with Hodgkin lymphoma, radiation therapy should be postponed until after delivery, if possible, to avoid any risk to the fetus.
Non-specific cutaneous symptoms may be treated with:
Hodgkin lymphoma can usually be cured if found and treated early. The prognosis of Hodgkin lymphoma has improved in recent decades, with a current 5-year survival rate of over 80%.
The prognosis depends largely on the following:
Cutaneous Hodgkin lymphoma usually represents advanced disease and carries a poor prognosis despite aggressive treatment [1].
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more