Authors:Zena Alani, Doctor and Clinical Researcher, New Zealand, 2022;
Dr Paul Jarrett, Dermatologist, Auckland, New Zealand, 2022.
Previous contributor:
Dr Amanda Oakley, Dermatologist, 2015.
Edited by theDermNet content department
Discoid lupus erythematosus (DLE) is a chronic scarring skin condition. It is the most common form of cutaneous lupus.
DLE is a sub-type of chronic cutaneous lupus erythematosus. It is characterised by persistentscalyplaques on the scalp, face, and ears which subsequently can progress to scarring, atrophy, dyspigmentation, and permanent hair loss in affected hair-bearing areas.
DLE can affect males and females of any age but occurs more frequently in women in their 20s, 30s, and 40s. Children are rarely affected. The estimated prevalence is around 20–40 people in every 100,000.
DLE is more common in skin of colour. For example, in New Zealand, Māori, and Pacific people have a significantly higher relative risk of discoid lupus erythematosus compared to the European population. This ethnic disparity has also been observed in the USA with those with skin of colour having an increased incidence of DLE.
What causes discoid lupus erythematosus?
The causes of DLE are endogenous and exogenous.
Endogenous factors include:
Geneticpredisposition with major histocompatibility complex allelesHLA-DQA1 and DRB1.
Single nucleotidepolymorphismTYK2, IRF5, CTLA4 are also associated.
Interferon, particularly type 1, is a key cytokine in pathogenesis.
IRF5 and TYK2 are involved in interferon regulation.
Smoking which is more common in those with DLE and which also impairs the efficacy of antimalarials
Ultraviolet radiation can provoke DLE as it is a photosensitive disorder. However, it can be found in non-sun exposed areas.
What are the clinical features of discoid lupus erythematosus?
DLE may be localised (above the neck in 80%) or generalised (above and below the neck in 20%). Often the rash is asymptomatic but it can be itchy and sore. Most patients with DLE only have skin involvement but some have or subsequently develop signs of SLE. Typically, the lesions evolve over time.
Typical signs of localised DLE include:
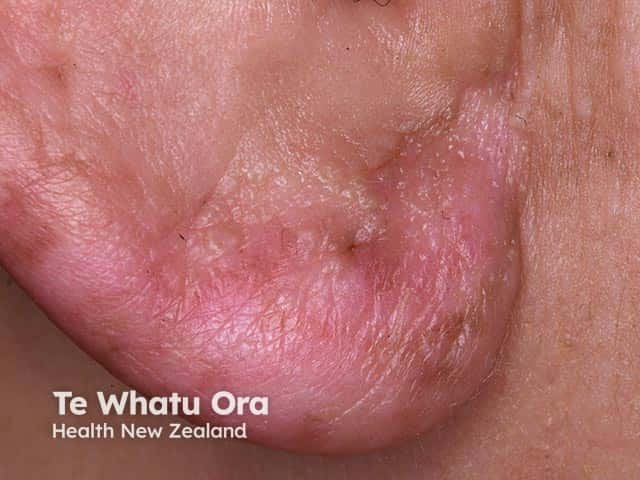
Initial dry red patches evolve to form red plaques with adherent scale.Follicularhyperkeratosis (plugs of keratin within hair follicles) is common. When this scale is removed using sticky tape the horny plugs can be seen giving rise to the “carpet-tack” sign.
As DLE progresses atrophic scarring and scarring alopecia is common. This is associated with hyper- and or hypo- pigmentary change and is especially noticeable in those with skin of colour.
DLE is typically located on the nose, cheeks, ear lobes, and conchal bowl (Shuster sign). It may involve lips, oral mucosa, nose, or eyelids.
Signs of generalised DLE include:
The morphology of the lesions is similar to that on the face and scalp but they are distributed widely including the anterior chest, upper back, dorsum of hands and less commonly on the lower limbs, palms, and soles. Rarely, there is involvement of the anogenital mucosa.
How do clinical features vary in differing types of skin?
DLE is more common in skin of colour. Hypo- and hyper-pigmentary change in those with skin of colour is especially noticeable and distressing.
What are the complications of discoid lupus erythematosus?
Discoid lupus erythematosus can have an impact physically and psychologically affecting the patient’s quality of life.
Dermatology Life Quality Index (DLQI) measures matched with Cutaneous Lupus Disease Area and Severity Index (CLASI) measures have shown that quality of life in patients with DLE is poor.
DLE commonly scars causing facial disfigurement and permanent alopecia. Pigmentary change may improve over long periods.
There is a link between DLE and systemic lupus erythematosus (SLE). Approximately 5% of patients with localised and 15% with generalised DLE develop SLE.
How is discoid lupus erythematosus diagnosed?
Discoid lupus erythematosus is diagnosed from its distribution and the clinical appearance of the plaques. A patient with DLE should undergo a complete examination for other manifestations of lupus.
A skin biopsy usually confirms diagnosis.
Features vary depending on the stage of the DLE but include an interfacedermatitis also involving hair follicles and a perivascular and peri-appendageal lymphocyticinfiltrate in the upper and lower dermis.
There is epidermal vacuolation and apoptoticbasal cells and hyperkeratosis.
The basement membrane may become thickened and dermalmucin may be present.
As lesions evolve further, the inflammatory infiltrate subsides and there is dermal fibrosis.
Blood tests include a full blood count, renal function, and antinuclear antibodies (ANA). ANA is frequently not detected.
Urine analysis.
What is the differential diagnosis for discoid lupus erythematosus?
What is the treatment for discoid lupus erythematosus?
General measures
Careful year-round protection from sun exposure using clothing and generously applied high SPF broad-spectrum sunscreens. Sunscreens alone are not adequate.
While indoors, some patients may also need to stay away from glass windows, or these can be treated with UV-blocking films.
Vitamin D supplements should be recommended for those who strictly avoid the sun.
Smoking cessation.
Specific measures
Local therapy
Intermittent courses of potent or ultrapotent topical corticosteroids applied for several weeks are the first treatment for localised DLE. Intralesional injections of corticosteroids are sometimes used.
Achtman JC, Werth VP. Pathophysiology of cutaneous lupus erythematosus. Arthritis Res Ther. 2015;17(1):182. Published 2015 Aug 10. doi:10.1186/s13075-015-0706-2. Journal
Albrecht J, Taylor L, Berlin JA, et al. The CLASI (Cutaneous Lupus Erythematosus Disease Area and Severity Index): an outcome instrument for cutaneous lupus erythematosus. J Invest Dermatol. 2005;125(5):889–94. doi:10.1111/j.0022-202X.2005.23889.x. Journal
Chen P, Broadbent E, Coomarasamy C, Jarrett P. Illness perception in association with psychological functioning in patients with discoid lupus erythematosus. Br J Dermatol. 2015;173(3):824–6. doi:10.1111/bjd.13709. Journal
Chong BF, Song J, Olsen NJ. Determining risk factors for developing systemic lupus erythematosus in patients with discoid lupus erythematosus. Br J Dermatol. 2012;166(1):29–35. doi:10.1111/j.1365-2133.2011.10610.x. Journal
Drenkard C, Parker S, Aspey LD, et al. Racial Disparities in the Incidence of Primary Chronic Cutaneous Lupus Erythematosus in the Southeastern US: The Georgia Lupus Registry. Arthritis Care Res (Hoboken). 2019;71(1):95–103. doi:10.1002/acr.23578. Journal
Gordon H, Chandran A, Vandal AC, Yung A, Jarrett P. The relationship between disease severity and quality of life in discoid lupus erythematosus. Br J Dermatol. 2017;177(4):1134–5. doi:10.1111/bjd.15227. Journal
Jarrett P, Thornley S, Scragg R. Ethnic differences in the epidemiology of cutaneous lupus erythematosus in New Zealand. Lupus. 2016;25(13):1497–1502. doi:10.1177/0961203316651745. Journal
Jessop S, Whitelaw DA, Grainge MJ, Jayasekera P. Drugs for discoid lupus erythematosus. Cochrane Database Syst Rev. 2017;5(5):CD002954. Published 2017 May 5. doi:10.1002/14651858.CD002954.pub3. Journal
O'Kane D, McCourt C, Meggitt S, et al. British Association of Dermatologists guidelines for the management of people with cutaneous lupus erythematosus 2021. Br J Dermatol. 2021;185(6):1112–23. doi:10.1111/bjd.20597. Journal