
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Clinical features
Diagnosis
Treatment
Propolis is the glue made by honeybees to build, repair and protect their hives. It consists of partially digested resins from a variety of tree buds and barks mixed with beeswax. In Europe, it derives mainly from poplar buds, but conifers are also used. Propolis, therefore, is a complex mixture comprising balsams and resins, waxes, essential oils, pollen and cinnamyl alcohol, vitamins A, B, C and E, flavonoids and minerals.
A number of other substances that are related to propolis may be listed as ingredients, particularly of cosmetics. Cera flava is the yellow wax produced from a honeycomb. Cera alba is the bleached form of Cera flava. It is used as an emulsifier and thickening agent in cosmetics and as a food additive (E901) for coating and glazing candy and fresh fruit. Other propolis-related substances include propolis cera, beeswax acid and synthetic beeswax.
Propolis is an increasingly important allergen, with European studies reporting positive patch test rates of 1.2 to 6.6%. In one series from Finland, the rate increased from 0.5% in 1995-7 to 1.4% in 2000-2. Another study in children reported an increase from 2% to 13.7% between 1995 and 2002; 75% of the patch test-positive children had used a natural product or alternative medicine remedy. In a 2010 Polish patch test study of children with chronic recurrent eczema and atopy, a positive propolis patch test was recorded in 16.5% of children aged 7-8 years and 5.4% of adolescents aged 16-17 years. Propolis was the second most common positive patch test allergen after nickel in children and the fourth most common in adolescents.
Paradoxically, contact stomatitis and allergic contact cheilitis to propolis have been reported in an HIV-positive patient taking a 30% propolis solution orally.
Exposure to propolis and propolis-related substances can occur in multiple settings.

Biocosmetics and biotherapeutics appear to be the most common source of exposure to propolis in those sensitised to it.
The major allergens in propolis derived from poplar buds are caffeates. 3-Methyl-2-butenyl caffeate and phenylethyl caffeate are the main sensitisers. Benzyl caffeate, geranyl caffeate, benzyl salicylate, benzyl cinnamate, methyl cinnamate, ferulic acid and tectochrysin are also sensitisers present in propolis.
Propolis allergy often cross-reacts with Myroxylon pereirae (balsam of Peru) as there are 13 known constituents in common. Other recognised cross-reactions due to shared ingredients (commonly cinnamic acid, cinnamyl alcohol, vanillin) include:
Crossreaction with beeswax is uncommon but can occur, possibly due to contamination with propolis.
Contact with propolis can be direct, or, less commonly, airborne.
Contact allergy to propolis results in dermatitis or urticaria. Symptoms and signs include:
Reactions begin within hours to days of exposure in a previously sensitised patient. Initial sensitisation takes 10–15 days.
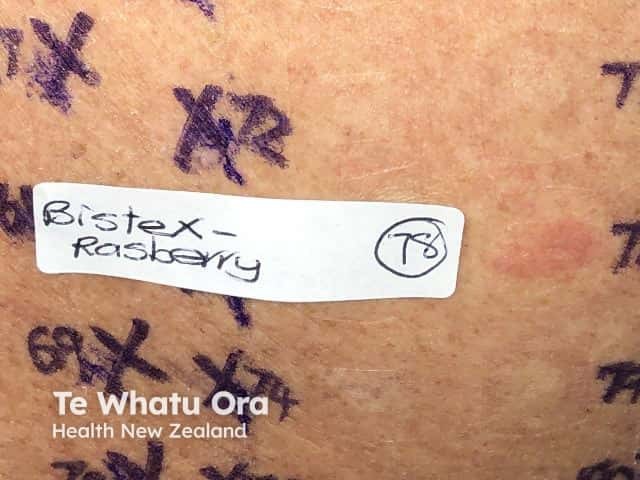
The diagnosis of propolis allergy is made by patch testing with propolis 10% in petrolatum and the likely source ‘as is’ or diluted eg honey, cosmetic or therapeutic formulation. A flare of original dermatitis has been reported in association with positive patch test reactions.

Avoidance of propolis-containing products results in resolution of the reaction, but sometimes a further unidentified source of propolis exposure causes persistence of milder symptoms. It is therefore important to re-assess should the contact allergy symptoms not settle completely despite avoidance of the original source of propolis.
Beekeepers with allergic contact dermatitis of the hands due to propolis may be able to continue working with hives by wearing rubber or leather gloves.
In one case, ingestion of propolis-enriched honey as a capsule had no effect despite cheilitis/perioral eczema and positive patch test to honey and propolis.
Patients with known allergies to conifer, poplar, salicylates and Myroxylon pereirae are advised to avoid propolis due to shared allergenic constituents. It is important to be aware of the names of propolis-related substances as these also should be avoided.
Dermatitis is usually treated with emollients and topical steroids; urticaria is treated with oral antihistamines.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more