Ocular rosacea: rosacea is an inflammatory disorder resulting in flushing, facial redness and spots
Infestation of the eyelash by Demodex mite (demodicosis)
Contact allergy to substances coming into direct contact with the lid margins, including rosin in mascara and preservatives in contact lens solutions.
Posterior blepharitis is the result of abnormalities of meibomian gland function in the inner eyelid. This gland normally produces oil, which is a component of the normal tear film. In blepharitis, the secretions from this gland thicken and block the gland.
Burning and foreign body sensation especially upon waking
Light sensitivity
It is also unsightly.
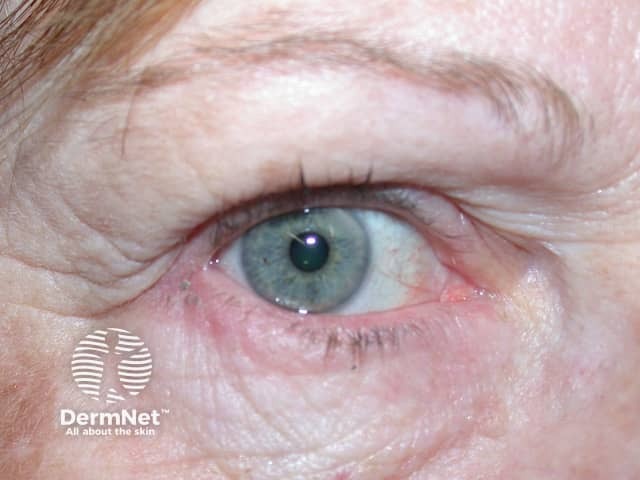
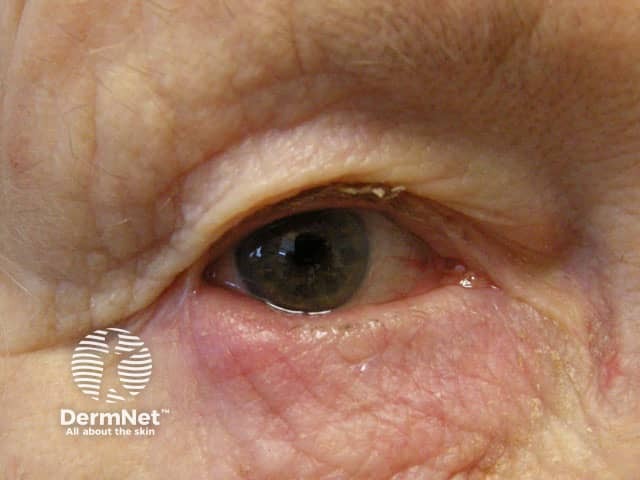
Red, swollen eyelid margins
Abnormal growth of eyelashes due to scarring of the eyelid margins
Flaking skin around the eyes resulting in matting of the lashes
Crusted eyelids
Scales may cling to the lashes
Frothy tear formation
What are the complications of blepharitis?
Complications from blepharitis include:
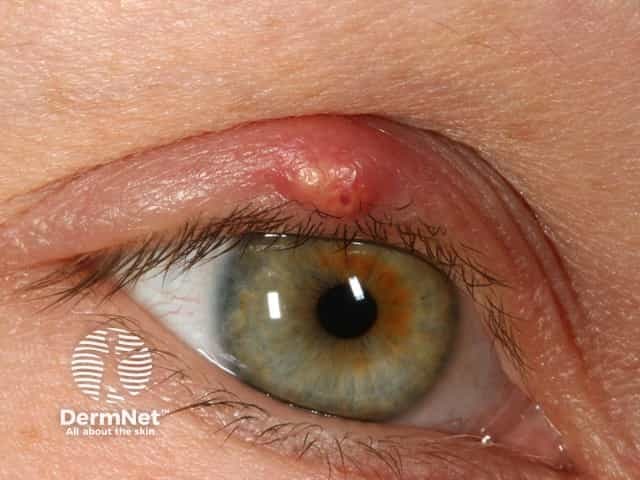
Stye (hordeolum) – a red tender lump caused by an infection of an oil gland of the eyelid.
Chalazion – a painless firm lump caused by inflammation of the oil gland of the eyelid. Chalazion can be painful and red if it becomes infected.
Abnormal or decreased oil secretion resulting in excess tearing or eye dryness.
Corneal infections due to abnormal or decreased oil secretion.
It is important to distinguish these from sebaceous carcinoma, a cancerous skin lesion that may rarely grow on eyelid skin.
Stye
Stye
Chalazion
How is blepharitis treated?
Treatment for blepharitis involves keeping good eyelid hygiene. Warm wet compresses applied to the eyelid will help to dislodge the crusts. The eyelid can be lightly scrubbed with a cotton swab using a mixture of water and baby shampoo.
In patients with posterior blepharitis, eyelid massage (firm presssure to the edge of the eylids at the base of the eyelashes) will help to clear the oil accumulated in the glands.
In severe cases of blepharitis, antibiotic or topical steroid eyedrops may be necessary. Where seborrhoeic dermatitis and rosacea are also present, these will need to be treated, usually with antifungal agents or oral tetracycline respectively.
References
Jackson WB. Blepharitis: Current Strategies In Diagnosis And Management. Can J Ophthalmol 2008 Apr;43(2):170-9.
Kanski JJ. Eyelids. In: Clinical Ophthalmology: A Systematic Approach. 4th edition. Boston ; Oxford : Butterworth-Heinemann1999: 9-12.