ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Outcome
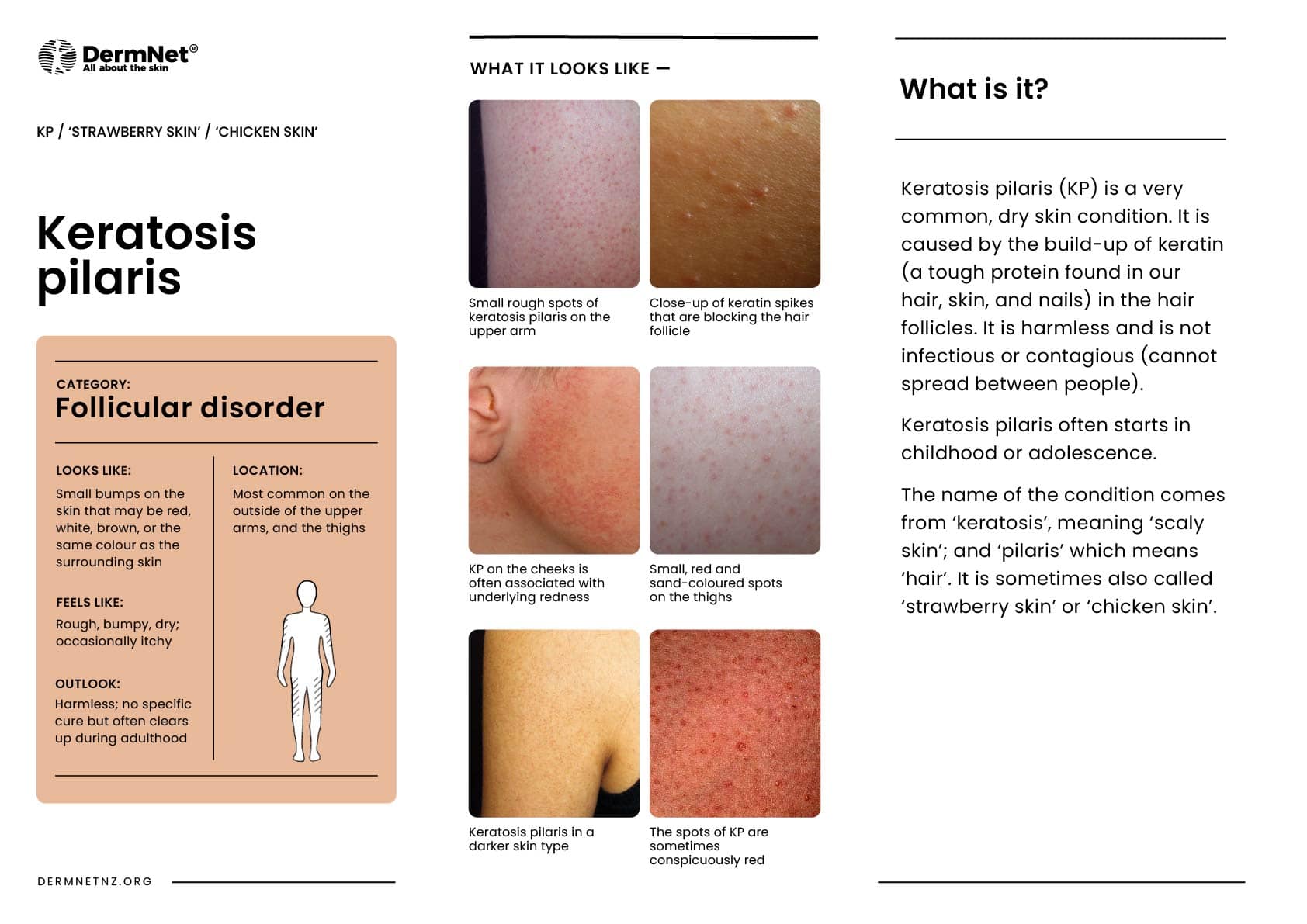
Keratosis pilaris is a very common, dry skin condition caused by keratin accumulation in the hair follicles.
The Latin term keratosis means ‘scaly skin’, and pilaris means ‘hair’. Keratosis pilaris usually starts in childhood but becomes more obvious during the teenage years and adulthood. It is harmless and is not infectious.



Keratosis pilaris is typically seen in children and young adults. It affects 50–70% of teenagers and 40% of adults. It has been associated with other skin diseases such as atopic eczema and ichthyosis.
Keratosis pilaris occurs due to abnormal keratinisation of the upper portion lining of the hair follicle. The keratin fills the follicle instead of exfoliating.
The cause of keratosis pilaris is not fully understood, but it is thought to have a genetic association with autosomal dominant inheritance. Correlations have been made with mutations in filaggrin (a key protein in skin barrier function).
Keratosis pilaris tends to be prominent in the winter months and is likely due to the reduced moisture content of the air.
Patients may complain about the ‘goosebump’ or ‘chicken skin’ appearance of their skin. These small bumps can be skin-coloured, red, or brown. The skin can feel rough, dry, and can occasionally be itchy. Redness can also be found around many of the small bumps.
Keratosis pilaris most commonly presents on the extensor surfaces of the upper arms and thighs. The buttocks, trunk, chest, face, and distal extremities can also be involved.
Keratosis pilaris may occasionally be associated with redness and pigmentation of the skin of the cheeks (erythromelanosis folllicularis facei et coli and keratosis pilaris rouge), loss of eyebrow hair (ulerythema ophryogenes), and small atrophic areas over the cheeks (atrophoderma vermiculatum).



The bumps are usually the colour of the patient’s skin. However, they can present as red areas on white skin or brown/black on darker skin.
Keratosis pilaris is a clinical diagnosis. Evaluation of the lesion can aid diagnosis:
There is no cure for keratosis pilaris, however, it often clears up during adult life. This is because adults tend to be better at managing the skin condition with the measures discussed above. Any atrophy or scarring with hair loss may be permanent.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more