ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Uses
Ingredients
How to use
Benefits
Side-effects and risks
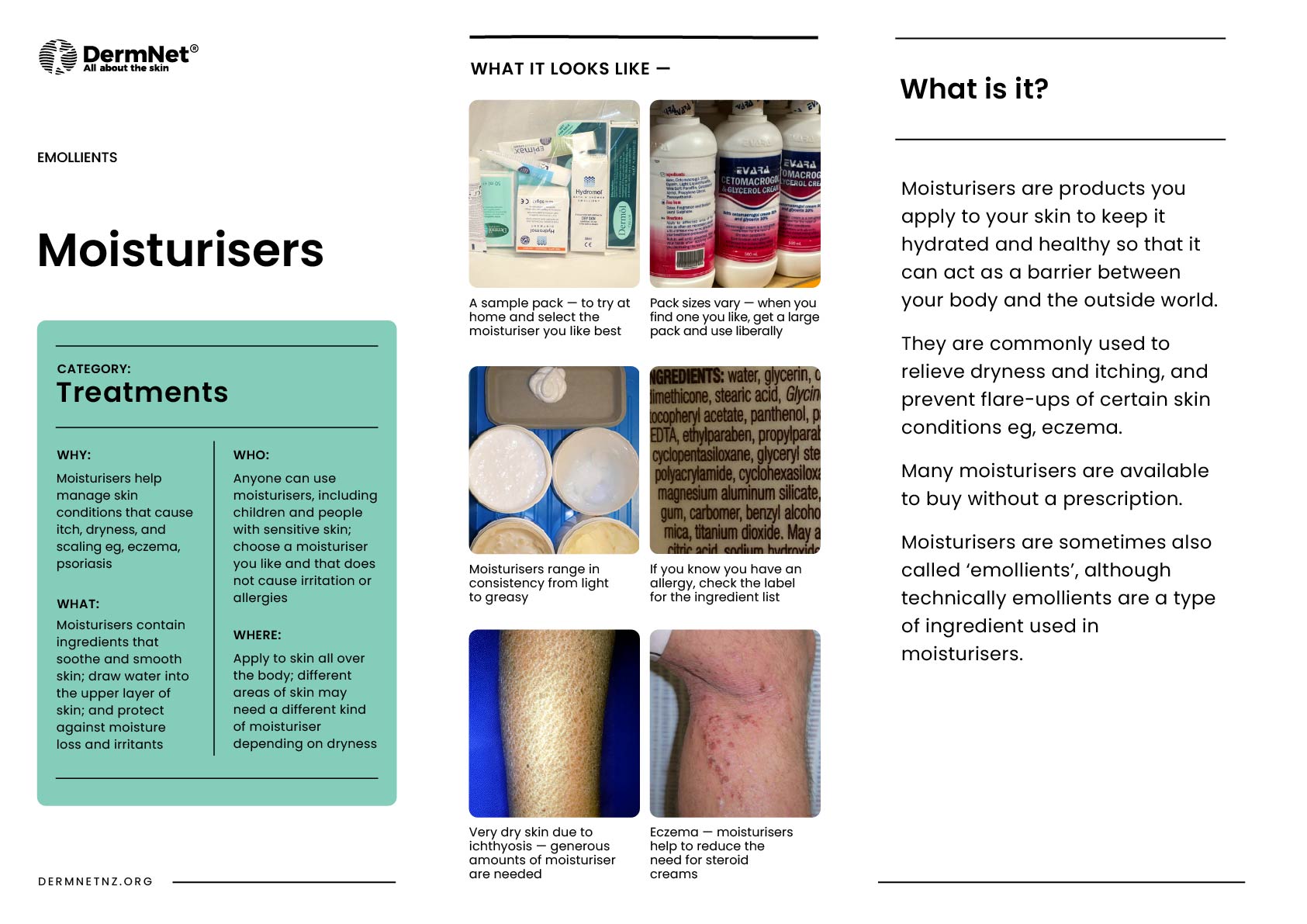
Moisturisers are products used to add moisture to the skin. Emollients are products used to soften and smooth skin (eg, lanolin, glycerol stearate). Although the terms emollient and moisturiser are often used synonymously, emollients can also be described as a specific ingredient of moisturisers.
There are often a number of available moisturisers. Options include:
Cetomacrogol and glycerine cream (sorbolene with glycerine) is a general-purpose moisturiser that is non-greasy, cheap, and available in bulk without prescription.


Uses of moisturisers include:
Components of moisturisers include emollients, occlusives, and humectants. Moisturisers may also contain other ingredients such as surfactants (cleansers), fragrances, and preservatives. Specially formulated products may also report antimicrobial, anti-itch, and anti-inflammatory actions.
The are various types of emollients available, these contain oily substances such as lanolin, glyceryl stearate, and soy sterols, that soften and smooth skin by filling cracks in the skin’s outermost layer.
Occlusive agents provide a hydrophobic (lipophilic) layer of oil on the surface of the skin, forming a protective barrier to reduce evaporative water loss from the stratum corneum (the outermost layer of the epidermis).
Examples of occlusive ingredients:
The following products are ordered from most to least occlusive:
Humectant agents are hydrophilic (‘water-loving’), therefore attract and retain water in the stratum corneum, similar to the natural hydrating factors found in corneocytes. They include:
Urea and other acidic preparations often sting if applied to scratched or fissured skin. They are also keratolytic, ie, they have a descaling or peeling effect, which is important in the management of ichthyosis.
Creams and lotions are prone to microbial contamination and preservatives (eg, parabens, formaldehyde-releasers, and isothiazolinones) are added to improve shelf life. Preservatives in moisturisers can lead to allergic contact dermatitis in sensitised individuals.
Many additional agents may be added to a moisturiser to appeal to the consumer. Be aware that marketing claims for these ingredients in reducing the signs of skin ageing can be misleading. Large molecules such as peptides and collagen cannot penetrate through the stratum corneum.
Application frequency and quantity is dependent on the severity of the dry skin:
People with sensitive skin associated with atopic dermatitis or rosacea often describe irritant reactions to moisturisers, such as burning and stinging. If irritation is transient, the product can generally continue to be used. It should be discontinued if contact dermatitis appears (see below).
Discontinue use if allergic contact dermatitis develops to a particular emollient or moisturiser. Suspected allergic contact dermatitis to particular preservatives, fragrances, or vehicles can be investigated by patch testing.
Occlusive emollients can cause or aggravate acne, perioral dermatitis, folliculitis, and boils.
Thermal burns from paraffin-containing ointments on clothing or bedding can be dangerous and can occur if ignited by cigarettes or naked flames.
Moisturising products (bath oils in particular) can be slippery and care should be taken while getting in and out of the bath or shower to avoid falls. Use of a bath mat may minimise this risk.
Approved datasheets are the official source of information for medicines, including approved uses, doses, and safety information. Check the individual datasheet in your country for information about medicines.
We suggest you refer to your national drug approval agency such as the Australian Therapeutic Goods Administration (TGA), US Food and Drug Administration (FDA), UK Medicines and Healthcare products regulatory agency (MHRA) / emc, and NZ Medsafe, or a national or state-approved formulary eg, the New Zealand Formulary (NZF) and New Zealand Formulary for Children (NZFC) and the British National Formulary (BNF) and British National Formulary for Children (BNFC).
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more