Pseudocarcinomatous hyperplasia can occasionally be observed in biopsies of CD30-positive lymphoproliferative disorders. It is important to be cognisant of this association, because epithelialhyperproliferation can overshadow large atypicallymphoid cells, leading to an erroneous diagnosis of squamous cell carcinoma or keratoacanthoma.
Histology of pseudocarcinomatous hyperplasia in anaplastic large cell lymphoma
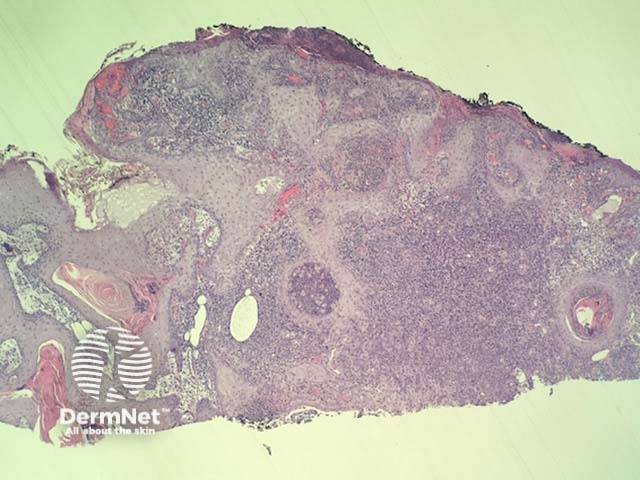
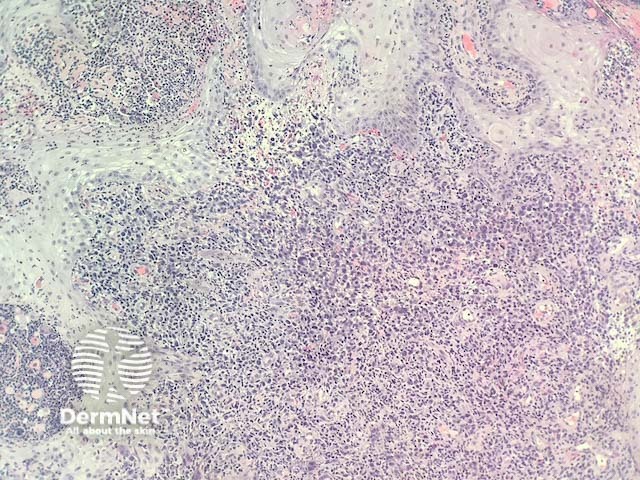
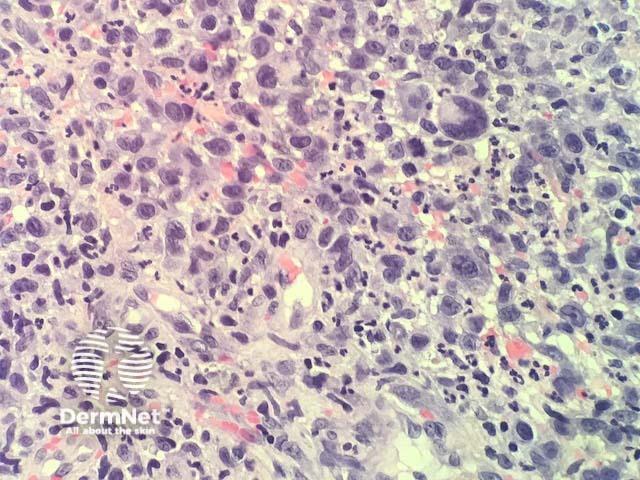
In pseudocarcinomatous hyperplasia in anaplastic large cell lymphoma, histopathology usually shows a cup-shaped keratinocyticproliferation with minimal cytologic atypia resembling a keratoacanthoma (figure 1). Directly adjacent to this proliferation, there is a dermaltumour composed of highly atypical large hematopoietic cells (figure 2,3).
Figure 1
Figure 2
Figure 3
Special studies for pseudocarcinomatous hyperplasia in anaplastic large cell lymphoma
Immunohistochemical studies reveal the dermal tumour is strongly positive with CD30. These cells show no positivity with p63 or CK5/6, which helps establish that these cells are not anaplastic squamous cell carcinoma cells. Melanoma markers are also negative in the dermal tumour cells.
Differential diagnosis for pseudocarcinomatous hyperplasia in anaplastic large cell lymphoma
Other diagnoses to be considered include:
Squamous cell carcinoma — immunohistochemical stains are usually needed to rule out dedifferentiation of squamous cell carcinoma (CK5/6, p63).
Melanoma immunohistochemical stains are usually needed to rule out dedifferentiation of melanoma (Sox-10, S100).
Systemic lymphoma — cutaneous involvement of a systemic lymphoma needs to be ruled out with clinical correlation.
References
Lin JH, Lee JY. Primary cutaneous CD30 anaplastic large cell lymphoma with keratoacanthoma-like pseudocarcinomatous hyperplasia and marked eosinophilia and neutrophilia. J Cutan Pathol 2004; 31: 458–61. PubMed