
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Signs and symptoms
Diagnosis
Differential diagnoses
Treatment
Prognosis
Mpox, formerly monkeypox, is a rare disease caused by the DNA monkeypox virus (MPV). The monkeypox virus belongs to the Orthopoxvirus genus — the same family of viruses as cowpox and smallpox. Infection with the MPV virus causes a rash similar to that of chickenpox.
Mpox gets its name from the discovery of the virus in monkeys under investigation in a research lab in Denmark in 1958. The first reported infection of humans was in the Democratic Republic of the Congo in 1970.
There are two principal strains (clades) of the mpox virus that produce sporadic outbreaks in Africa (numbering 1 to 2 thousand cases a year); a more virulent strain in the Congo basin and a milder strain in West Africa. In endemic areas, most sufferers are thought to acquire the disease from exposure to infected animal carcasses, meat, or blood (animal-to-human transmission). The average age at presentation has increased in the last two decades from 4 to 21 years. The disease is most frequent in the Democratic Republic of the Congo (DRC).
Isolated outbreaks outside Africa have mostly been related to infected animal importation but person-to-person spread has increased via direct contact with body fluids, large respiratory droplets, and contaminated linen and bedding being implicated in transmission.
From late July 2022 to May 2023, the world health organisation (WHO) labelled mpox a public health emergency of international concern. The majority of cases (86%) were from the European region (approx. 2900 cases) followed by the Americas (approx. 380), African region (73), Eastern Mediterranean Region (15), and Western Pacific Region (11). Person-to-person spread is evident from close physical proximity or sexual activity, predominantly in men who have sex with men. So far all cases have been linked to the less virulent West African strain. Fomites may be an important mode of transfer from active mpox lesions.
In August 2024, WHO once again declared mpox a public health emergency of international concern. This was in response to the growing number of mpox cases in the DRC and other African countries (Rwanda and Kenya). To date, the responsible variant is clade 1b; it seems to be more infectious than the clade 2 variant in the 2022 outbreak, spreading readily by both sexual and casual skin contact in both adults and children. Alarmingly the mortality rate seems to be higher, with 4 in 100 cases resulting in death. Mass vaccination in high infection areas is being considered at press.
The disease may become more common since administration of the smallpox vaccine, which confers cross-protection, was discontinued in the 1970s.
The incubation period from infection to prodromal symptoms of mpox is 12 days.
In the first 5 days of the infection, patients experience 'flu-like' symptoms including:
After this period, a rash similar to that seen in chickenpox develops:
The rash begins as 2–5 mm diameter maculopapules, which evolve into:
Symptoms usually last for 14 to 21 days; the rash lasts for approximately 10 days.
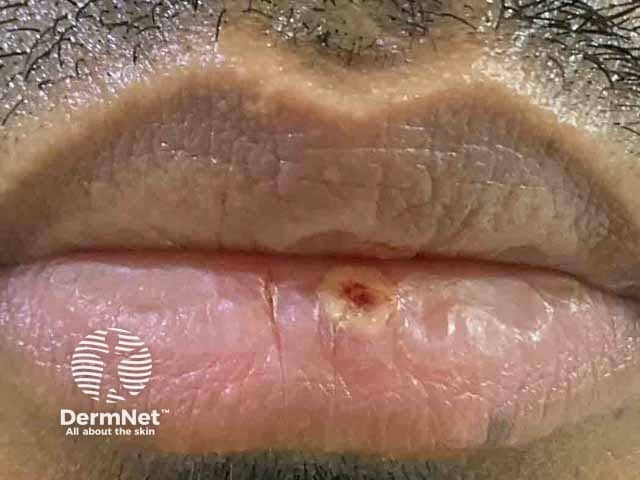
A large series of sufferers from the 2022 outbreak in Spain were reported at the time of writing (August 2022). Many of those affected were men, and had few lesions (less than 20 in total), often only in a single area. Lesions often started on the genitals, face, arms, hands, and perianal area.
Rather than true pustules, pseudo-pustules, which were solid, white, and raised without a top layer that could be scraped off to release pus, were described. Pseudo-pustules are extremely rare in other infections and this is a crucial diagnostic sign. Lesions progressed to small areas of skin necrosis then ulcers; finger lesions produced mpox whitlows. Scarring may occur. Rarely the illness is preceded by a morbilliform eruption.





The prodromal features, coupled with the development of lymphadenopathy, and the chickenpox-like rash should alert suspicion. Unlike chickenpox, lesions may be present on the dorsal hands and feet, palms, and soles.
Virological confirmation can be made by:
With the increased awareness of person-to-person transmission, particularly during the 2022 outbreak, cases should be isolated and contact tracing initiated. Close contacts of infected individuals require isolation for 21 days.
Supportive symptomatic treatment (treatment of secondary infection, pneumonia, and corneal infection) may be needed.
Specific antiviral therapy with cidofovir or a newer agent, tecovirimat may be indicated in those at high risk, or those with severe disease.
Very young patients, malnourished patients, pregnant women, and the immunocompromised may suffer more severe disease.
Smallpox vaccination offers significant protection (85%) against the related monkeypox virus; the risk-benefit of vaccination should be considered for high-risk contacts. Newer two-dose Ankara strain vaccinations have been licensed for prevention of mpox since 2019 in the United Kingdom. It can be administered as post-exposure prophylaxis preferably within 4 days of exposure
In recent years, the mortality of Mpox has ranged from 3–6%, with infants and the immunocompromised having higher mortality.
There were no deaths in the 2003 USA outbreak, and severe illness requiring hospitalisation only occurred in 2 young children.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more