Author: Dr Amanda Oakley, Dermatologist, Hamilton, New Zealand, 1997. Updated by Dr Anita Eshraghi, Dermatologist, Sweden. February 2018. Revised September 2020
Miliaria is a common skin disease caused by blockage and/or inflammation of eccrine sweat ducts. Miliaria is frequently seen in hot, humid, or tropical climates, in patients in hospital, and in the neonatal period. Miliaria is also known as heat rash, sweat rash or prickly heat.
Based on the level of the sweat duct obstruction, miliaria is divided into three types:
Miliaria crystallina (sudamina) is due to obstruction of the sweat ducts close to the surface of the skin in the stratum corneum of the epidermis
Miliaria rubra follows obstruction of the sweat ducts in the deeper layers of the skin (mid-epidermis)
Miliaria profunda (tropical anhidrosis) is the result of sweat leaking from the sweat glands into the middle layer of skin (blockage at or below the dermoepidermal junction) following repeated episodes of miliaria rubra.
Miliaria
Miliaria
Who gets miliaria?
Miliaria crystallina affects up to 9% of neonates, with the mean age of 1 week. It can also occur in adults with fever.
Miliaria rubra is the most common type of heat rash. It is seen in children and in up to 30% of adults who move to a tropical environment or are unexpectedly exposed to heat and humidity. Although miliaria may develop within days of arriving in the tropics, it often takes several months to peak.
Miliaria profunda is rare and presents in adult males.
Heat rash can affect all age groups and racial groups.
What causes miliaria?
Prickly heat results from sweating. The main contributing causes and risk factors are:
Immature sweat ducts in a newborn child
A hot and humid environment
Intense exercise or physical activity
Fever
Occlusion of the skin with non-porous dressings or synthetic clothing against the skin
Hospitalised or bedridden patients lying on waterproofed mattresses or mattress-protectors.
Other diseases and treatments that have been associated with miliaria are:
Genetic disease (Morvan syndrome and pseudohypoaldosteronism type I)
Radiotherapy.
What are the clinical features of miliaria?
Symptoms of heat rash vary depending on type:
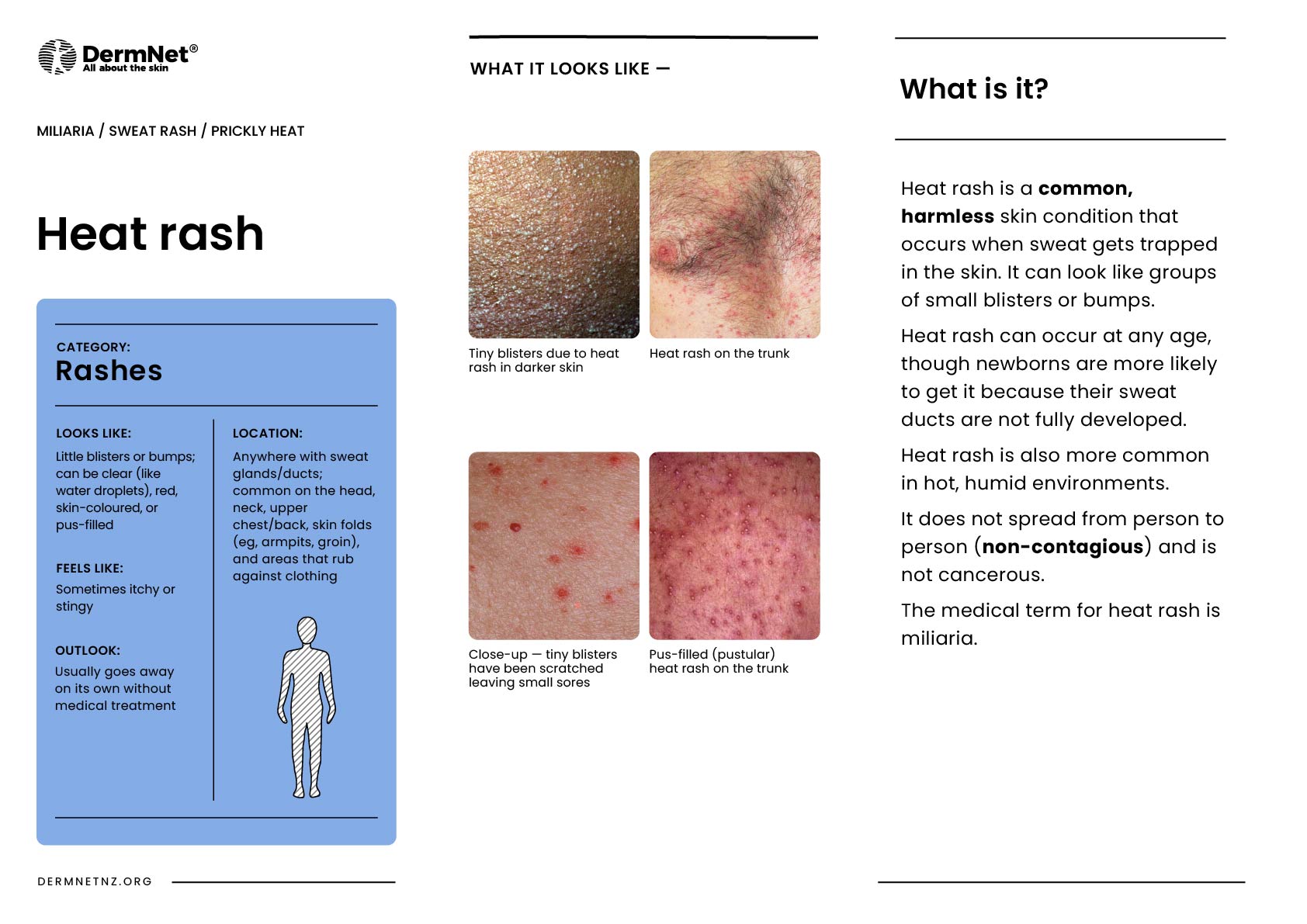
Miliaria crystallina presents as 1–2 mm superficial clear blisters that easily break. The blisters can look like beads of sweat. There is no inflammation. The blisters are usually seen widely spread on the head, neck, and upper trunk. The vesicles break easily to leave a bran-like scale.
Miliaria rubra, the most common form of heat rash, results in red, 2–4 mm, non-follicularpapules and papulovesicles. They are very itchy. Background erythema is often present. In children, miliaria involves the trunk and the skin folds of the neck, axilla or groin. In adults, miliaria often affects the upper trunk, scalp, neck and flexures, particularly in areas of friction with clothing.
Miliaria pustulosa is a variant of miliaria rubra with pustules.
Miliaria profunda presents as asymptomatic deep papules. The flesh–coloured, 1–3 mm diameter papules develop on the trunk and extremities.
Heat rash is diagnosed on its typical clinical presentation.
In severe cases or repeated episodes, punch biopsy can be useful. Miliaria crystallina shows vesicles associated with the sweat ducts within or just under the stratum corneum of the epidermis. Histology of miliaria rubra shows spongiosis and spongiotic vesicles.
Tzanck smear taken from vesicles will distinguish miliaria from herpes simplex or toxic erythema of the newborn.
What is the differential diagnosis for miliaria?
Skin disorders presenting with papules, vesicles, or pustules that look similar to miliaria include:
Resolution of miliaria requires minimising heat and humidity to reduce sweating and the avoidance of irritation to the skin. Strategies to avoid sweating, keeping the skin cool, and reducing irritation can help treat and prevent heat rash:
Work in an air-conditioned office for at least a few hours a day
Sleep in a ventilated, cool bedroom
Move away from a tropical climate, avoiding humid weather
Avoid excessive clothing and tight clothing
Avoid excessive soap and irritants
Wear shirts and blouses made of breathable synthetic fabrics or cotton
Remove wet clothing
Cool water compresses and taking a cool bath
Patients should be education on symptoms of heat exhausation.
Heat rash may require medical care which can involve:
Calamine lotion to relieve discomfort; because calamine lotion is drying, an emollient may be required.
Treatment of fever with antipyretic such as paracetamol (American terminology acetoaminophen)
Most cases of heat rash resolve within a day or two after changing to a cooler environment without any treatment or complications.
References
Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004;29(1):32–4. doi:10.1111/j.1365-2230.2004.01444.x.PubMed.
Carter R 3rd, Garcia AM, Souhan BE. Patients presenting with miliaria while wearing flame resistant clothing in high ambient temperatures: a case series. J Med Case Rep. 2011;5:474. doi:10.1186/1752-1947-5-474. PubMed Central.
Godkar D, Razaq M, Fernandez G. Rare skin disorder complicating doxorubicin therapy: miliaria crystallina. Am J Ther. 2005;12(3):275–6. PubMed
Nguyen TA, Ortega-Loayza AG, Stevens MP. Miliaria-rash after neutropenic fever and induction chemotherapy for acute myelogenous leukemia. An Bras Dermatol. 2011;86(4 Suppl 1):S104–6. doi:10.1590/s0365-05962011000700027. PubMed.
Miller JL. Diseases of the eccrine and apocrine sweat glands. In: Bolognia JL, Schaffer J, Cerroni L (eds). Dermatology [2 volumes], Elsevier, 2017.