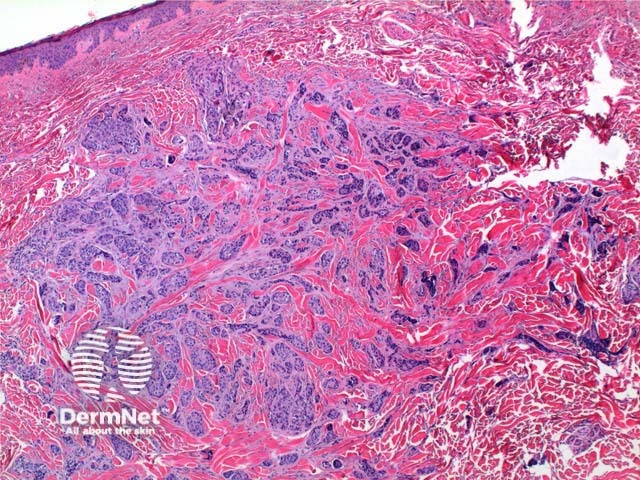
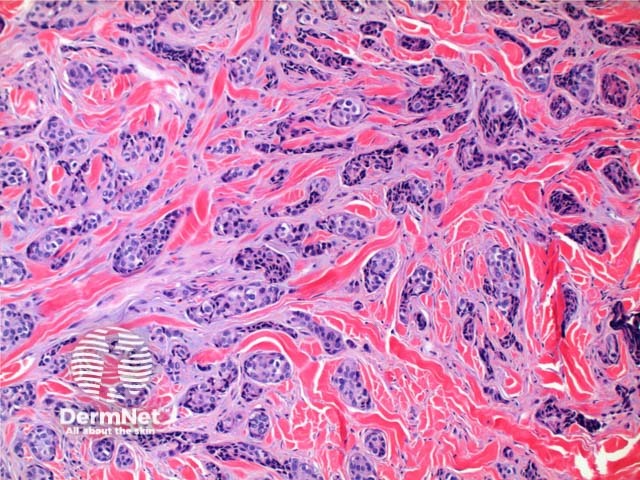
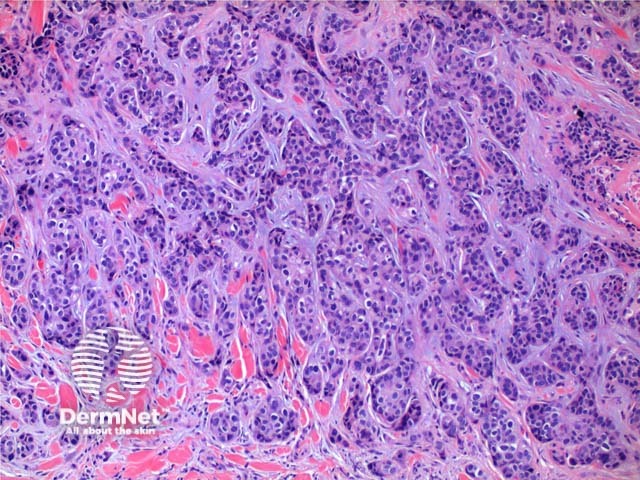
The histology of metastaticadenocarcinoma may show a number of patterns. Low power view frequently shows a poorly circumscribed infiltrating tumour centred on the dermis (Figure 1). Cords and nodules of atypicalepithelial cells can be seen dissecting between collagen bundles (Figure 2). These may show evidence of duct or gland formation (Figure 3), and may be set in a mucinous stroma (Figure 4). Vascular and lymphatic permeation may be evident in the telangiectoides and erysipeloides variants of breast metastases.
Figure 1
Figure 2
Figure 3
Figure 4
Special stains and differential diagnosis of metastatic adenocarcinoma
While there is no substitute for clinical correlation and staging investigations, immunohistochemistry can provide clues to the site of origin, and help discriminate from primarycutaneousadnexaltumours. While never entirely specific, general rules are outlined below.
P63: Positive more commonly in primary cutaneous adnexal tumours.
CK7-/CK20+: Suggestive of gastrointestinal origin
CK7+/CK20-: Suggestive of lung origin
CK7: Focal staining suggestive of primary cutaneous adnexal tumour vs strong and diffuse staining in metastatic adenocarcinoma
CK 5/6: Negative staining infrequently seen in primary cutaneous tumours
CDX2: Suggests gastrointestinal origin
Villin: Gastrointestinal, pancreatic or biliary origin.
ER, PR and GCDFP: Favour breast origin. Note that all have been seen expressed in primary adnexal tumours and metastatic lesions can lose staining ability.
Mammaglobin: Diffuse staining favours metastatic breast. Scattered positivity can be seen in primary cutaneous adnexal tumours.
PSA and prostatic acid phosphatase: Support prostatic origin
Podoplanin (D240): Negative staining suggests a metastatic lesion
References
Book: Skin Pathology (2nd edition, 2002). Weedon D
Book: Pathology of the Skin (3rd edition, 2005). McKee PH, J. Calonje JE, Granter SR
Plaza JA, Ortega PF, Stockman DL, Suster S. Value of p63 and podoplanin (D2-40) immunoreactivity in the distinction between primary cutaneous tumors and adenocarcinomas metastatic to the skin: a clinicopathologic and immunohistochemical study of 79 cases. J Cutan Pathol. 2010;37(4):403–10. doi:10.1111/j.1600-0560.2010.01517.x. PubMed
Fernandez-Flores A. Mammaglobin immunostaining in the differential diagnosis between cutaneous apocrine carcinoma and cutaneous metastasis from breast carcinoma. Cesk Patol. 2009;45(4):108–12. PubMed
Azoulay S, Adem C, Pelletier FL, Barete S, Francès C, Capron F. Skin metastases from unknown origin: role of immunohistochemistry in the evaluation of cutaneous metastases of carcinoma of unknown origin. J Cutan Pathol. 2005;32(8):561–6. doi:10.1111/j.0303-6987.2005.00386.x. PubMed
Cangelosi JJ, Nash JW, Prieto VG, Ivan D. Cutaneous adnexal tumor with an unusual presentation--discussion of a potential diagnostic pitfall. Am J Dermatopathol. 2009;31(3):278–81. doi:10.1097/DAD.0b013e31819ddccf. PubMed
Plumb SJ, Argenyi ZB, Stone MS, De Young BR. Cytokeratin 5/6 immunostaining in cutaneous adnexal neoplasms and metastatic adenocarcinoma. Am J Dermatopathol. 2004;26(6):447–51. doi:10.1097/00000372-200412000-00001. PubMed