
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Causes
Demographics
Signs and symptoms
Diagnosis
Treatment
Complications
Prevention
Meningococcal disease is an illness caused by the bacteria Neisseria meningitidis. The two common presentations of meningococcal infection are meningococcal meningitis (infection of the membranes that surround the brain and spinal cord) and meningococcemia (infection of the bloodstream). An infected individual may suffer one or both of these diseases.
Meningococcal disease is a medical emergency and patients showing signs and symptoms suspicious of meningococcal infection need to seek medical advice from their doctor or a hospital immediately. A delay of even hours can be fatal. There are several deaths from meningococcal disease every year in New Zealand and even more during epidemics.
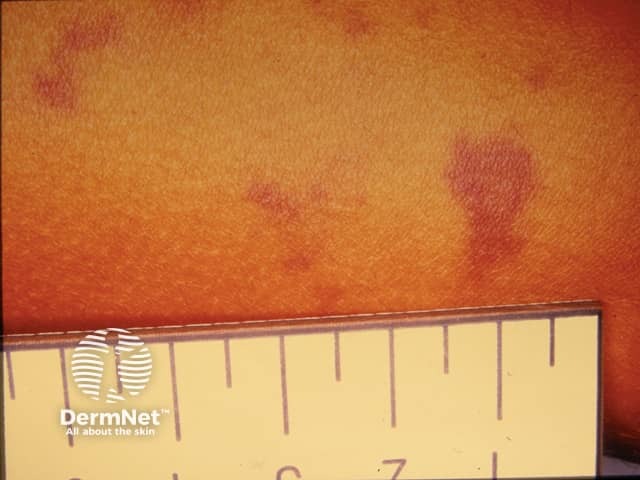
The most common cutaneous sign of meningococcal disease is localised acral purpura.



Neisseria meningitidis bacteria are spread from person to person by inhaling airborne droplets when an infected person coughs or sneezes or just by close contact.
In many cases, the bacteria is spread by infected individuals that are carriers of Neisseria meningitidis but do not show any symptoms. Neisseria meningitidis is present in the nose and throat of these individuals, but the body's natural defence mechanisms contain the infection by producing antibodies against the bacteria so that spread to other parts of the body is prevented. Carrier rates depend on age and the highest rate is found in young adults (15-24 years) at 20-40%.
Rarely, exposure to Neisseria meningitidis will lead to meningococcal disease where bacteria spreads to the blood and brain, causing meningococcemia and/or meningococcal meningitis. This may occur if the body has not had enough time to build up an antibody defence or in those with defective immune systems.
Most patients with meningococcal disease are otherwise healthy individuals. However, there are some patient groups who are at an increased risk for developing a meningococcal infection.
The most common signs and symptoms of meningococcal disease are listed below.
If an individual has both meningococcal meningitis and meningococcaemia, they may present with a mixture of symptoms and signs characteristic to each of the diseases.
Children >1 year and adults:
Infants:
Signs on the skin:
Other signs and symptoms:

Meningococcal meningitis and meningococcemia is often suspected from the history and physical examination. Blood culture and/or lumbar puncture are used to confirm the diagnosis. A lumbar puncture involves putting a needle in the lower back to obtain some cerebrospinal fluid (CSF). An increased number of white cells are seen under the microscope, with meningitis confirmed when the leukocyte count in the CSF is > 5 cells/µL (bacterial meningitis often has >1000 cells/µL, with neutrophilic predominance). Microscopy (a Gram stain showing Gram-negative diplococci), culture and polymerase chain reaction (PCR) for meningococcus will confirm the diagnosis.
Patients suspected of raised intracranial pressure or with a focal neurological deficit may undergo CT scanning.
Early recognition of meningococcal infection is critical as meningococcemia spreads so quickly that within hours of symptoms appearing, a patient may rapidly die. Patients may initially just have a rash and not be particularly unwell. Meningococcemia can kill more rapidly than any other infectious disease. Patients with either meningococcemia or meningococcal meningitis must be hospitalised and treated with antibiotics and supportive care immediately. Many patients are admitted to an intensive care unit.
Penicillin is the drug of choice. Some strains of Neisseria meningitidis are resistant to penicillin have been isolated; in these cases, third-generation cephalosporins are a suitable alternative. Very sick patients are often treated with both penicillin and cephalosporins prior to obtaining the laboratory results.
Other treatments may include:
Patients who survive very severe cases of meningococcemia may have suffered severe necrosis (cell death) of skin and underlying tissue. Skin grafts and amputation may be necessary.
Complications from meningococcal disease may occur at the time of the acute disease or during the recovery period. Some complications are so severe that they may reduce the chances of survival.
There are two ways to prevent meningococcal disease. One is by immunisation with vaccines (immunoprophylaxis) and the other is giving antibiotic therapy to close contacts of patients with meningococcal disease (antimicrobial chemoprophylaxis).
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more