Maculopapular mastocytosis in adults is unlikely to resolve with time. It may rarely lead to systemic involvement, where the mastocytosis spreads to more than one tissue.
Histology of maculopapular cutaneous mastocytosis
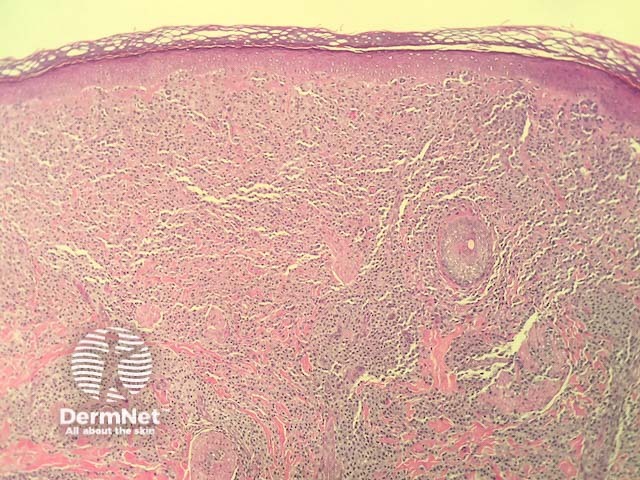
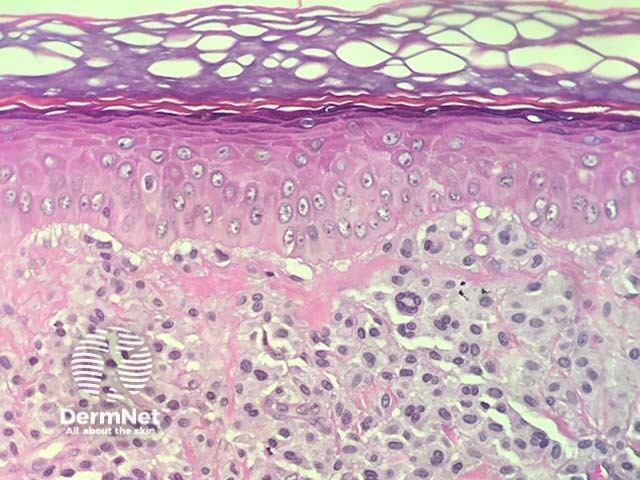
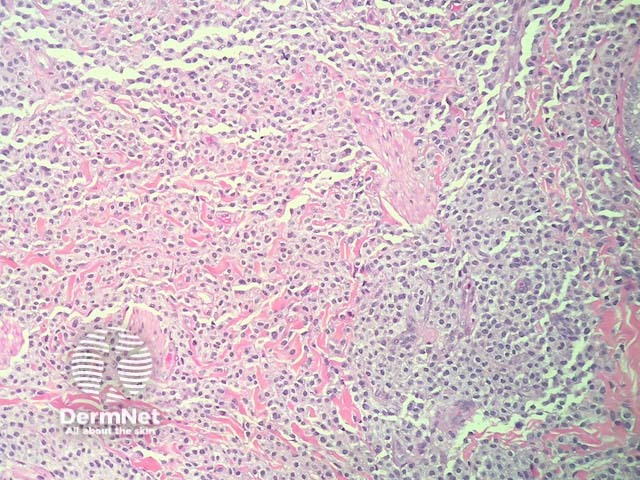
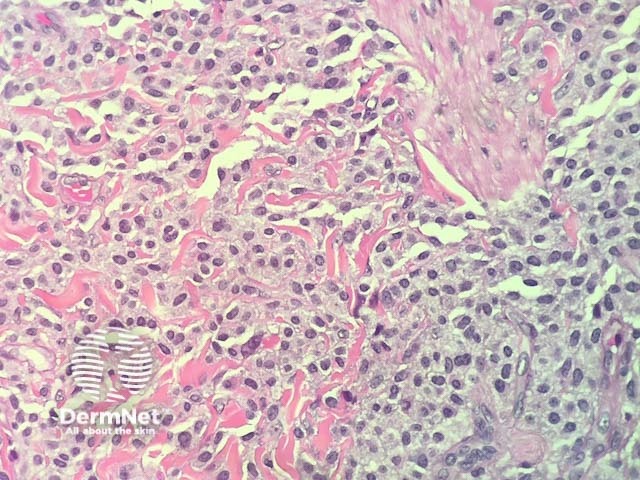
In maculopapular cutaneous mastocytosis, the histopathology shows an accumulation of mast cells in the dermis (figures 1-4). Mast cells are round or spindle shaped with abundant eosinophiliccytoplasm which contain minute granules, distinct cytoplasmic boundaries, and large pale nuclei (best seen in figures 2-4). Often there are accompanying other inflammatory cells including histiocytes, eosinophils and lymphocytes. There may be oedema of the dermis, particularly if the lesion has been traumatised.
Figure 1
Figure 2
Figure 3
Figure 4
Special studies for maculopapular cutaneous mastocytosis
Giemsa, toluidine blue , tryptase, and Leder special stains can help highlight the mast cells. Immunohistochemistry with CD117 is very helpful in difficult cases, as this nicely highlights the mast cells.
Differential diagnosis for maculopapular cutaneous mastocytosis
Other diagnoses to be considered include:
Langerhans cell histiocytosis — this disease can have a similar morphology and clinical presentation. In Langerhans cellhistiocytosis immunohistochemistry will demonstrate the cells are positive with CD1a instead of CD117
Urticaria — the infiltrate may include some mast cells but typically there are many more neutrophils, eosinophils and spare infiltrates around vessels.
References
Kelly JV. Generalized, well-dispersed rash · wheal development after tactile irritation · normal vital signs · Dx? J Fam Pract. 2015 Oct;64(10):645–7. PubMed PMID: 26551471.