Dowling-Degos disease is an autosomal dominant skin disorder characterised by progressivepigmentation of the skin within body folds. Association with loss-of-function mutations in KRT5 (encoding keratin 5) is documented.
Histology of Dowling-Degos disease
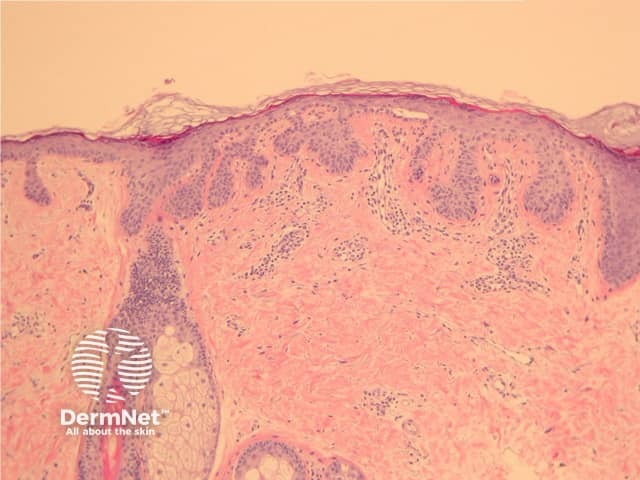
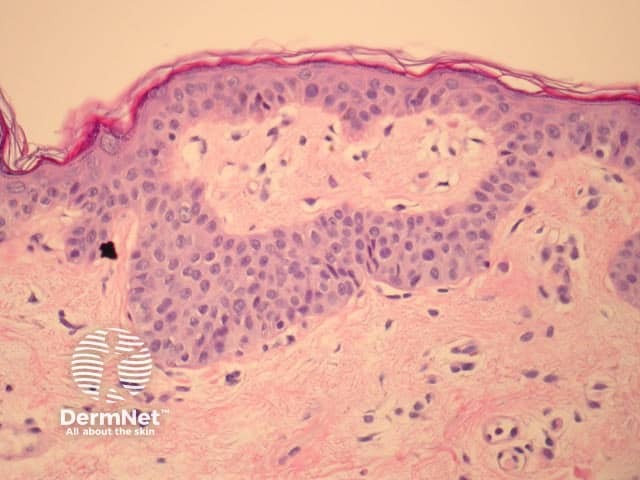
Epidermal changes in Dowling-Degos disease include hyperkeratosis, often with small horncysts and thinning of the suprapapillary epidermis. Thin epithelial strands extend into the superficial dermis from the epidermis and hairfollicles resulting in an ‘antler-like’ pattern (Figures 1, 2). Epidermal hyperpigmentation is usual although rare non-pigmented variants are reported. The hair follicleinfundibulum may be dilated. Dermalperivascularlymphohistiocyticinfiltrate (figures 1,2,3) or a lichenoid tissue reaction pattern may be seen.
Figure 1
Figure 2
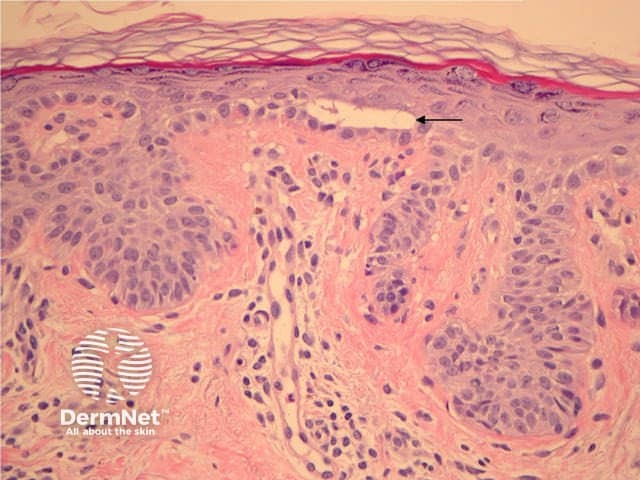
Figure 3
Differential diagnosis of Dowling-Degos disease
Galli-Galli disease is a subtype of Dowling-Degos disease and is distinguished by the additional finding of non-dyskeratoticacantholysis (Figure 3, arrow). Other clinical and histological features are identical to Dowling-Degos disease.
Seborrhoeickeratosis — in Dowling-Degos disease, epithelial strands extend from the epidermis and hair follicles. The clinical presentation is very helpful in differentiating these conditions.
Haber syndrome — shared histological features with Dowling-Degos disease; however, the clinical presentation is distinct with facial rosacea-like lesions, pitted scars and seborrhoeic keratosis-like lesions in the trunk and flexures. Haber syndrome is not associated with keratin 5 mutations.