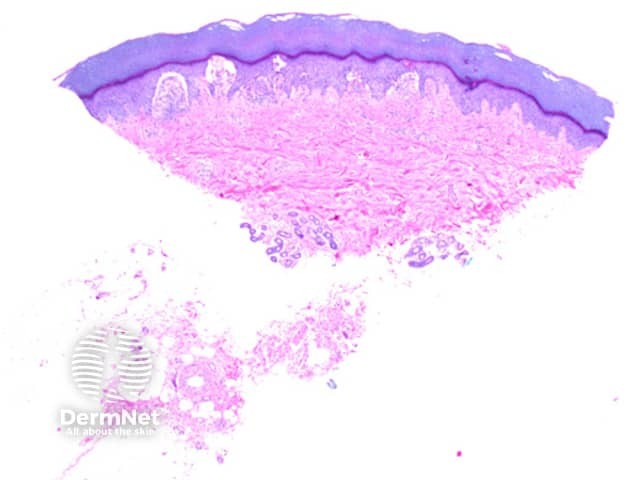
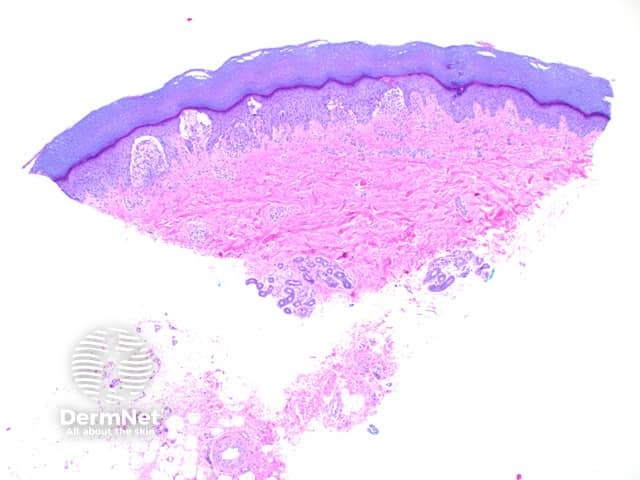
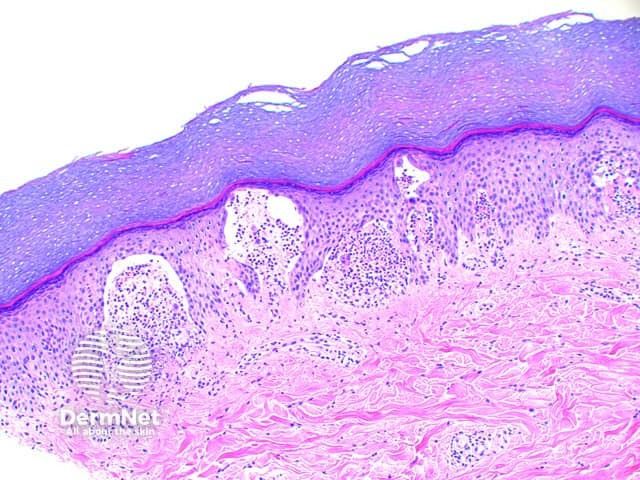
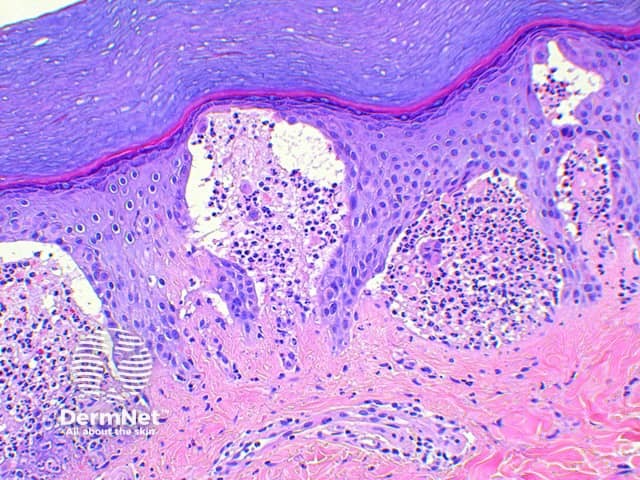
Scanning power view of dermatitisherpetiformis shows vesicular reaction pattern (Figure 1), characterized by foci or small zones of subepidermal separation (Figures 2 and 3). Dense clusters of neutrophils and scattered eosinophils fill the papillary dermis forming microabscesses (Figure 4). Acantholytickeratinocytes may also be evident within the papillary microabscess (Figure 4). With time the small areas of papillary dermal separation may join to form larger areas of vesiculation.
Figure 1
Figure 2
Figure 3
Figure 4
Variants of dermatitis herpetiformis
Pemphigus herpetiformis: Strictly a variant of pemphigus, it is mentioned here as it may present as a clinical mimic of dermatitis herpetiformis. The histology is that of pemphigus, typically foliaceous type, with formation of intraepidermalvesicles.
Special stains in dermatitis herpetiformis
Direct immunofluorescence studies show granular deposits of IgA in the dermal papillae.
Differential diagnosis of dermatitis herpetiformis
Herpes virus infection: Despite the occasional presence of acantholytic keratinocytes, dermatitis herpetiformis does not show multinucleation, nuclearchromatin changes or cellularinclusions.
Linear IgA bullousdermatosis: The histological findings are largely identical, though acantholysis and fibrin at the tips of the dermal papillae and leukocytoclasis is more common in dermatitis herpetiformis. The immunofluorescence findings will show a linear basement membrane IgA staining.
Bullous lupus erythematosus: The histology may be identical with discrimination only possible where linear IgG and IgM is found at the basement membrane. Deposits of IgA can also be seen concurrently. Frequently the dermal papillary neutrophilicinfiltrate is seen to extend into the surrounding interstitium.
Cicatricial pemphigoid: In early lesions papillary abscess formation can be seen, though the eosinophilic population increases with lesion time. The key distinguishing feature is the presence of dermal scarring beneath the blister. Immunofluorescence also differs with linear IgG typically seen at the basement membrane. Exceptional cases may show IgA deposition alone.
References
Skin Pathology (3rd edition, 2002). Weedon D
Pathology of the Skin (3rd edition, 2005). McKee PH, J. Calonje JE, Granter SR
Am J Dermatopathol. 1983 Dec;5(6):547–54. Histology of linear IgA disease, dermatitis herpetiformis, and bullous pemphigoid. Blenkinsopp WK, Haffenden GP, Fry L, Leonard JN. PubMed
An Bras Dermatol. 2011 Jul-Aug;86(4 Suppl 1):S92–5. Bullous systemic lupus erythematosus: differential diagnosis with dermatitis herpetiformis. Barbosa WS, Rodarte CM, Guerra JG, Maciel VG, Fleury Júnior LF, Costa MB. PubMed