
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction Demographics Causes Health problems due to aeroallergen Investigation How to minimise reactions Treatment
Aeroallergens are various airborne substances or inhalants, such as pollens, spores, and other biological or non-biological airborne particles that can cause allergic disorders. Inhalation or cutaneous contact with aeroallergens can trigger a release of proteins in the form of an allergic reaction on the skin and mucous membranes [1,2].
Airborne particles can also cause irritant reactions without causing an immunological response.
The most common aeroallergens causing disease are pollens and house dust mites. Pollens are derived from:
Other aeroallergens may include:
Combustion product irritants include:
Allergies only affect susceptible individuals (see DermNet's page Allergies explained) whereas irritant reactions can affect anyone.
The prevalence of aeroallergens is quite variable from one region or country to another, depending on the climate, the local plants and animals, and the degree of pollution [3,4].
Climate change has been reported to contribute to the rise of some types of aeroallergens and to a surge in allergic disorders [5–7].
In New Zealand, the main aeroallergens are grasses [8]. The pollen season lasts for about 34 weeks beginning in July or August.
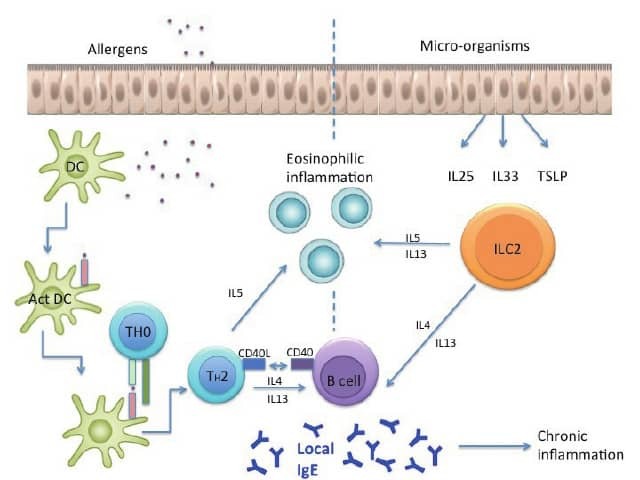
Although usually due to other factors, some common skin conditions are occasionally triggered or aggravated by aeroallergens [9–11]. How this occurs remains unclear (see figures 1 and 2 below for proposed mechanisms).
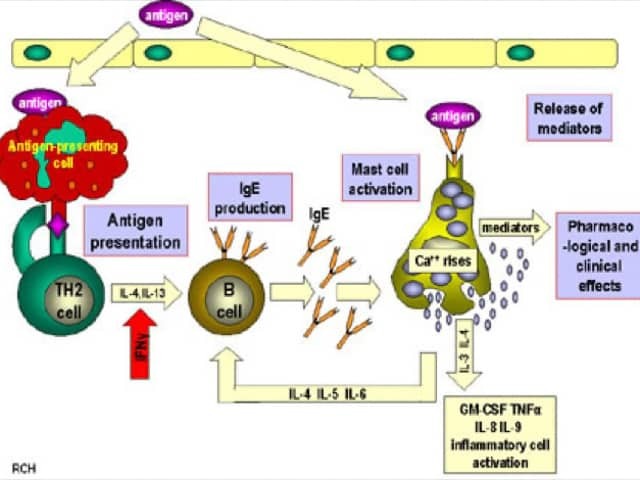
Credit: Ghaffar A, Hunt R. Immunology. Chapter seventeen: Hypersensitivity reactions. Microbiology and Immunology On-line. [14].
Aeroallergens commonly cause allergic rhinitis, allergic conjunctivitis, and allergic asthma, and they may contribute to eosinophilic oesophagitis [14–16].
Skin conditions due to aeroallergens are less common. These include:



When a careful patient history and examination findings lead to suspicion of a cutaneous reaction to aeroallergens, investigations may include:
The avoidance and elimination of aeroallergen triggers can be challenging.
Be aware of the allergenic plants in your region and monitor the local pollen forecast. Stay indoors and consider taking antihistamines and other medications when the pollen count is high.
Thoroughly clean contaminated areas such as bathrooms, laundries, and basements. Ventilate damp areas to prevent the growth of moulds.
Clean and vacuum all pillows, mattresses, bed-sheets, towels, carpets, and upholstered furniture. Consider using pillow and mattress protectors to minimise house dust mites.
Avoid contact with animals if possible. Bathe pets regularly.
The treatment of an aeroallergen allergic disease depends on the symptoms experienced.
Immunotherapy for allergic diseases (whether serial subcutaneous injections or sublingual) can reduce the reaction to aeroallergens in some patients.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more