ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Causes
Clinical features
Complications
Diagnosis
Treatment
Prevention
Outlook
Actinic keratosis is a precancerous scaly spot found on sun-damaged skin, also known as solar keratosis. It may be considered an early form of cutaneous squamous cell carcinoma (a keratinocyte cancer).



Actinic keratoses affect people that have often lived in the tropics or subtropics and have predisposing factors such as:
However, even in temperate climates they may be common - in southern Ireland and northwest England up to 25% of people aged 60 years and over have at least one.
Actinic keratoses are the result of abnormal skin cell development due to DNA damage by short wavelength UVB.
They are more likely to appear if the immune function is poor, due to ageing, recent sun exposure, predisposing disease, or certain drugs.
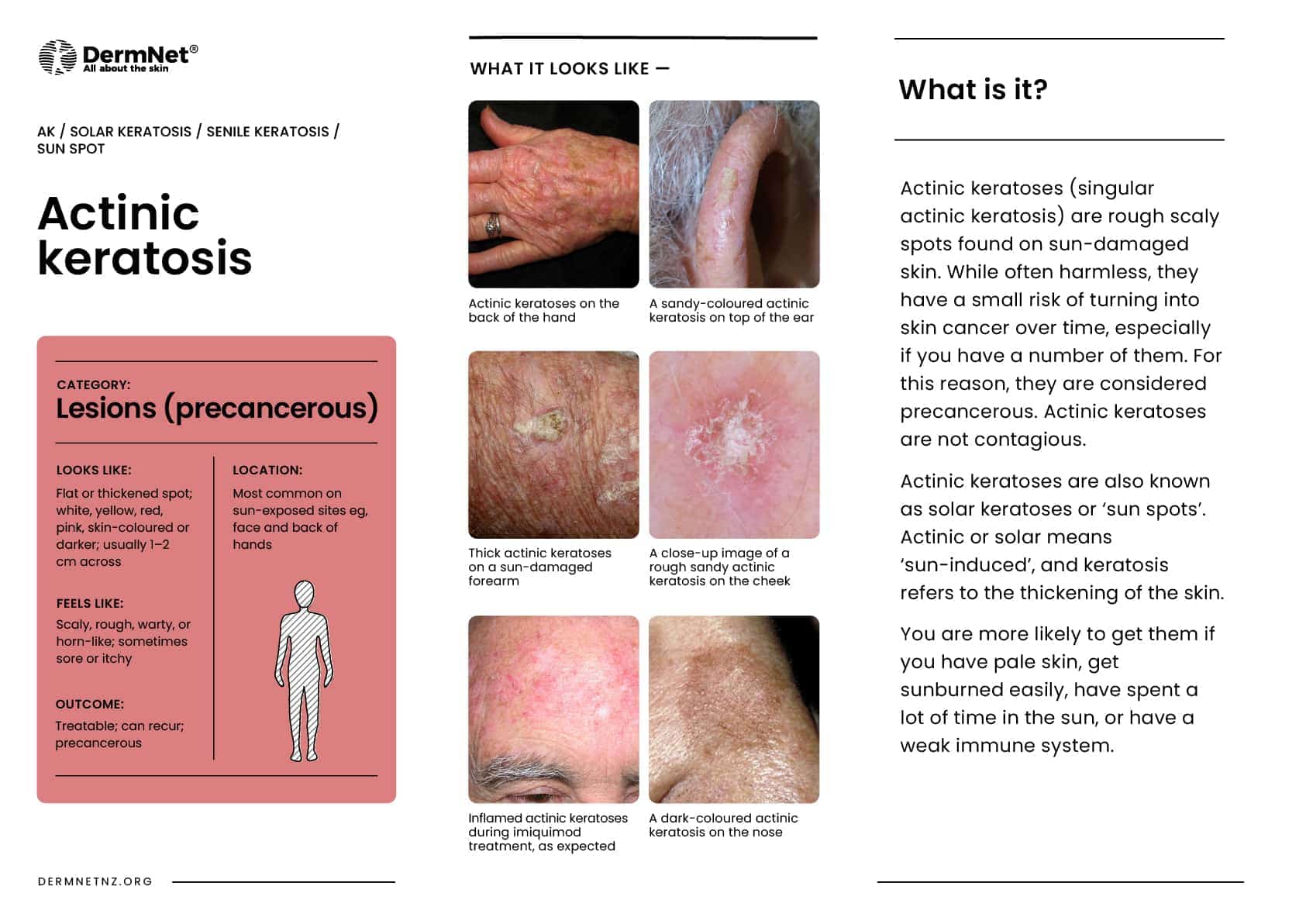
Actinic keratosis may be solitary but there are often multiple keratoses. The appearance varies.
They are sometimes graded according to their appearance:
Grade 1: Mild pink or grey marks with slight scale and gritty to touch
Grade 2: Moderate thicker hyperkeratosis and easily detected
Grade 3: Severe hyperkeratotic thick keratin
Grade 4: Confluent areas several centimetres with a range of the above grades of AK
Actinic keratoses are very common on sites repeatedly exposed to the sun, especially the backs of the hands and the face, most often affecting the ears, nose, cheeks, upper lip, vermilion of the lower lip, temples, forehead, and balding scalp. In severely chronically sun-damaged individuals, they may also be found on the upper trunk, upper and lower limbs, and dorsum of feet.



Many more images of actinic keratoses ...
The main concern is that actinic keratoses indicate an increased risk of developing cutaneous squamous cell carcinoma. It is rare for a solitary actinic keratosis to evolve to squamous cell carcinoma (SCC), but the risk of SCC occurring at some stage in a patient with more than 10 actinic keratoses is thought to be about 10 to 15%. A tender, thickened, ulcerated, or enlarging actinic keratosis is suspicious of evolution to SCC.
Cutaneous horn may arise from an underlying actinic keratosis or SCC.
Because they are sun damaged, people with actinic keratoses are also at risk of developing actinic cheilitis, basal cell carcinoma (BCC, which is more common than SCC), melanoma, and rare forms of skin cancer such as Merkel cell carcinoma.
Actinic keratosis is usually easy to diagnose clinically or by dermoscopy (see actinic keratosis dermoscopy). Occasionally, a biopsy is necessary, for example, to exclude SCC, or if treatment fails.
Actinic keratoses are usually removed because they are unsightly or uncomfortable, or because of the risk that skin cancer may develop in them. The latter point is a matter of considerable debate, and the most robust studies (Cochrane review) did not find convincing evidence that AK treatment resulted in a prevention of invasive squamous cell carcinomas.
Treatment of an actinic keratosis requires removal of the defective skin cells. Epidermis regenerates from surrounding or follicular keratinocytes that have escaped sun damage.
Some AKs will resolve with the frequent and appropriate use of sunscreens.
Tender, thickened, ulcerated, or enlarging actinic keratoses should be treated aggressively. Asymptomatic flat keratoses may not require active treatment but should be kept under observation.
Physical treatments are used to destroy individual keratoses that are generally symptomatic or have a thick hard surface scale. The lesions may recur in time, in which case they may be retreated by the same or a different method.
Liquid nitrogen spray is required to achieve adequate depth and duration of the freeze. This varies according to lesion location, width, and thickness. Healing varies from 5–10 days on the face, 3–4 weeks on the hands, and 6 weeks or longer on the legs. A light freeze for a superficial actinic keratosis usually leaves no mark, but longer freeze times result in hypopigmentation or scar.
Shave, curettage (scraping with a sharp instrument) and electrocautery (burning) may be necessary to remove a cutaneous horn or hypertrophic actinic keratosis. Healing of the wound takes several weeks or longer, depending on the body site. The specimen is sent for histological examination.
Excision ensures the actinic keratosis has been completely removed, which should be confirmed by pathology. The surgical wound is sutured (stitched). The sutures are removed after a few days, the time depending on the size and location of the lesion. The procedure leaves a permanent scar.
Creams are used to treat areas of sun damage and flat actinic keratoses, sometimes after physical treatments have been carried out. Field treatments are most effective on facial skin. Pretreatment with keratolytics (such as urea cream, salicylic acid ointment or topical retinoid), and thorough skin cleansing improves response rates. Results are variable and the course of treatment may need repeating from time to time. With the exception of diclofenac gel, field treatments all result in local inflammatory reactions such as redness, blistering and discomfort for a varying length of time.
Actinic keratoses are prevented by strict sun protection. If already present, actinic keratoses may improve with a very high sun protection factor (50+) broad-spectrum sunscreen applied at least daily to affected areas, year-round.
The number and severity of actinic keratoses can also be reduced by taking nicotinamide (vitamin B3) 500 mg twice daily.
Alpha-HPV vaccination may reduce the number of AKs in immunocompetent individuals with multiple AKs.
Actinic keratoses may recur months or years after treatment. The same treatment can be repeated or another method used. Patients who have been treated for actinic keratoses are at risk of developing new keratoses. They are also at increased risk of other skin cancers, especially intraepidermal squamous cell carcinoma, invasive cutaneous squamous cell carcinoma, basal cell carcinoma and melanoma.
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more