
ADVERTISEMENT
You do not have any notes added to this page yet
Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Outcome
Subcutaneous fat necrosis of the newborn (SCFN) is a rare, self-limiting panniculitis that usually appears as firm, inflamed skin-coloured to purple nodules (lumps) in the first few days of life. Lesions most commonly appear on the thighs, buttocks, cheeks, back, and arms.



SCFN is most common in term and postterm newborns, however, some cases have been described in premature neonates. Cases tend to be observed within the first 4 weeks of life.
The pathophysiology of SCFN is unclear but it is thought to mainly affect the brown fat, which is high in saturated fatty acids and has a role in heat generation in response to cold exposure. Under stress, tissue hypoxia with impaired perfusion leads to the crystallisation of subcutaneous fat tissues, resulting in tissue necrosis and clinical features of SCFN of the newborn.
Predisposing risk factors:
It is important to be aware that most neonates who are exposed to the above factors do not get SCFN.
Tender, firm, rubbery, red nodules typically appear on the back, buttocks, shoulders, cheeks, and extremities. Nodules size can range from singular lesions 1cm to multiple lesions >8cm in diameter. In some instances, particularly on the back and buttocks, broad areas of fat necrosis can occur and manifest as large plaques.
Nodules may be woody hard on palpation and as they progress may develop a brown colour. Larger nodules may become fluctuant in nature. Patients are often afebrile and without systemic symptoms.
SCFN of the newborn is less severe than sclerema neonatorum, which is another condition that may cause hardened skin in newborns.
Subcutaneous fat necrosis of the newborn can manifest as darkened/pigmented nodules or plaques rather than erythematous appearance.
The nodules of subcutaneous fat necrosis of the newborn are often painful and in rare cases may last for months before resolving. Occasionally, the infant may be left with a dimpled area of reduced fat.
Hypercalcemia is a rare but serious complication of SCFN. This is due to increased prostaglandin activity, released calcium from necrotic fat, raised macrophage secretion of 1,2-dihydroxycolecalciferol, and decreased renal calcium clearance. All babies with subcutaneous necrosis of the newborn should have blood calcium checked periodically for the first few months of life.
Signs and symptoms of hypercalcemia include:
Subcutaneous fat necrosis of the newborn has been associated with long-term thrombocytopenia. Infrequently, infants may also exhibit thrombocytosis. Anaemia, low blood sugar level (hypoglycaemia), and raised levels of fat in the blood (hyperlipidaemia) have also been observed.
In most cases, these laboratory abnormalities occur early in the disease course and are mild and transient.
Subcutaneous fat necrosis of the newborn is usually diagnosed clinically. Biopsy of skin can be performed to confirm the diagnosis.
Histopathology findings include:
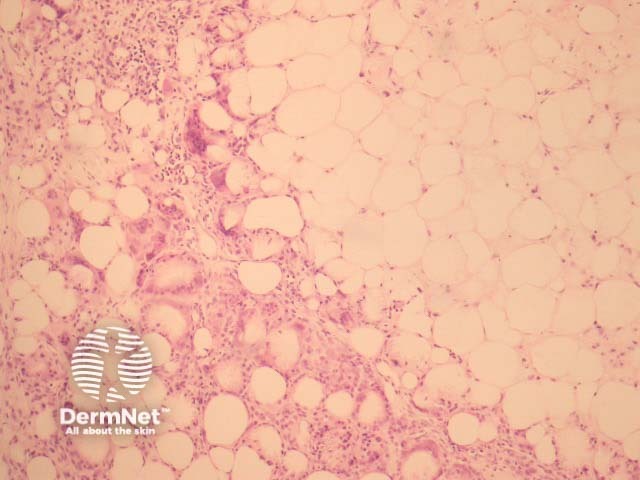
Ultrasound can be used to confirm the diagnosis, and does not require sedation or the use of ionising radiation.
SCFN is generally self-limiting and management should focus on symptom control. The inflammation often settles without specific treatment. If severe, systemic corticosteroids can be used to control the inflammation.
Hypercalcaemia secondary to subcutaneous fat necrosis of the newborn may require treatment such as increasing fluid intake, low calcium milk feeds, furosemide, corticosteroids, and bisphosphonates. Monitoring of blood calcium levels (for at least 4 months) is recommended.
The prognosis is usually favourable and treatment is unnecessary.
Subcutaneous fat necrosis of the newborn — The Australasian College of Dermatologists
An AI summary will appear based on your search term using data from all of the topic pages across the entire DermNet site.
Show more